
Journal of Integrative Medicine & Therapy
Download PDF
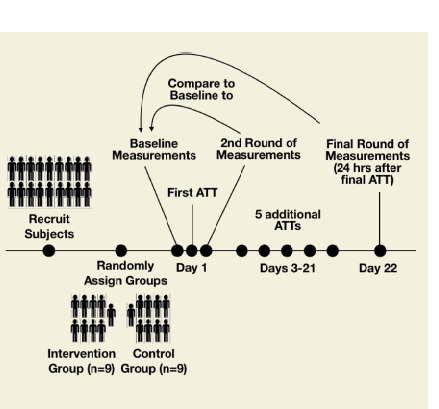 Figure 1: Experimental design.
Figure 1: Experimental design. 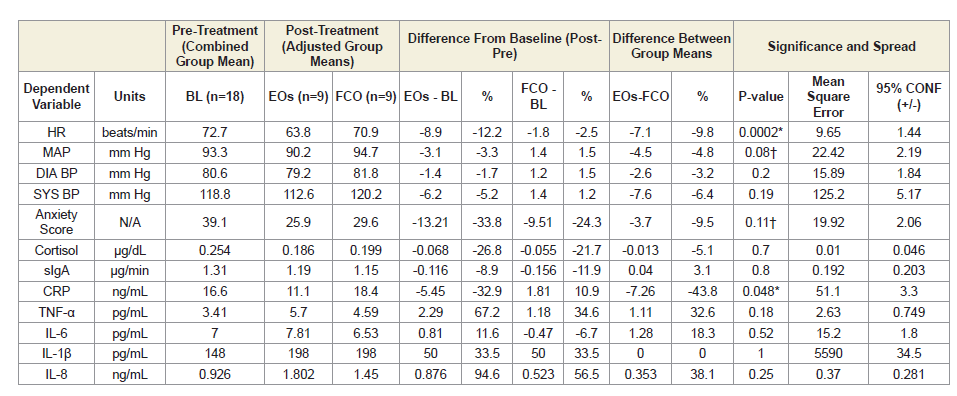 Table 1: Immediate effects of the AromaTouch Technique with or without essential oils.
Table 1: Immediate effects of the AromaTouch Technique with or without essential oils. 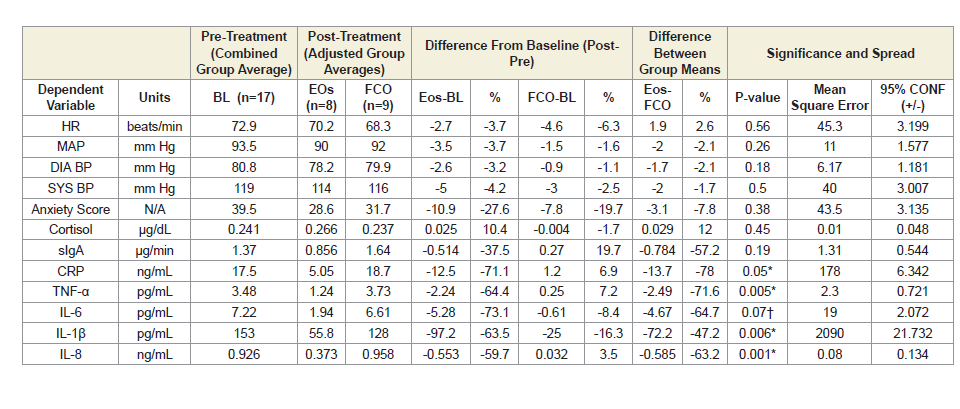 Table 2: Lasting effects of the AromaTouch Technique with or without essential oils.
Table 2: Lasting effects of the AromaTouch Technique with or without essential oils.
Research Article
Immediate and Lasting Effectsof the dōTERRA AromaTouch Technique®, a Topical Essential Oil Application Procedure, on Autonomic Function and Salivary Biomarkers: A Pilot Trial
Tyler Bahr*, Damian Rodriguez and Kathryn Allred
- dōTERRA International, LLC, USA
Address for Correspondence: Tyler Bahr, dōTERRA International, LLC, 389 S 1300 W, Pleasant Grove, UT 84062, USA, E-mail: tbahr@doterra.com
Citation: Bahr T, Rodriguez D, Allred K. Immediate and Lasting Effects of the dōTERRA AromaTouch Technique, a Topical Essential Oil Application Procedure, on Autonomic Function and Salivary Biomarkers: A Pilot Trial. J Integrative Med Ther. 2018;5(1): 7.
Journal of Integrative Medicine & Therapy | ISSN: 2378-1343 | Volume: 4, Issue: 1
Submission: 27 April, 2018| Accepted: 30 May, 2018 | Published: 08 June, 2018
Copyright: © 2017 Bahr T, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Objectives: To explore the immediate and lasting benefits of the essential oils used in the dōTERRA AromaTouch Technique®, an essential oil application method similar to a full-body aromatherapy massage, on stress, immune secretions, inflammatory signaling, and anxiety in healthy volunteers.
Design: Pilot trial.
Location: dōTERRA International corporate campus (Pleasant Grove, UT).
Subjects: Healthy volunteers (n=18).
Interventions: Half of the subjects (n=9) received the technique twice per week for three weeks. Control groups consisted of the other healthy individuals (n=9) who received the same massage-like technique with fractionated coconut oil instead of the essential oils.
Outcome Measures: Salivary levels of cortisol (μg/dL), TNF-α (pg/mL), IL-6 (pg/mL), IL-1β (pg/mL), IL-8 (ng/mL), and C-reactive protein (ng/mL) as well as the secretory rate of immunoglobulin A (μg/min), heart rate (beats/minute), blood pressure (mm Hg), and Spielberger state anxiety scores. Baseline measurements were taken immediately before the first session. Additional measurements were taken immediately after the first session and after receiving bi-weekly sessions for a 3-week period.
Results: Both groups experienced decreases in heart rate, mean arterial pressure, diastolic blood pressure, state anxiety scores, and salivary levels of cortisol immediately after the first session. The essential oil group also showed significantly decreased levels of C-reactive protein in the saliva immediately after the technique. After three weeks of regularly receiving the technique, subjects in the essential oil group had significantly lower salivary levels of C-reactive protein and three of the four inflammatory cytokines tested.
Conclusions: Because of the experimental design, many outcomes of the technique can be attributed specifically to the activity of the essential oils. The essential oils used in the AromaTouch Technique may be effective for enhancing the relaxation associated with a massagelike procedure involving physical touch. The oils in the technique may also be solely responsible for a major inhibitory effect on inflammatory signaling. Validation of this result warrants further investigation in a trial with a larger sample size.
Keywords
AromaTouch Technique; Essential oils; dōTERRA; Aromatherapy massage; Anti-inflammatory activity; pro-inflammatory cytokines; C-reactive protein
Abbreviations
EO(s): Essential oil(s); ATT: AromaTouch Technique®; FCO: Fractionated Coconut Oil; SYS: Systolic; DIA: Diastolic; BP: Blood Pressure; HR: Heart Rate; MAP: Mean Arterial Pressure; ANS: Autonomic Nervous System; CRP: C-Reactive Protein; SSAI: Spielberger State Anxiety Inventory; sIgA: Secretory IgA
Introduction
Aromatherapy, the inhalation or topical use of essential oils [EOs] for therapeutic benefit, and massage have been investigated separately and in combination with positive results on various patient populations. These results are largely due to the relaxing effects of EOs on the autonomic nervous system [ANS] and their antiinflammatory properties. There is evidence that EOs and their aromas decrease heart rate and blood pressure in both healthy individuals and individuals with heart rate variability, anxiety, or chronic stress [1,2]. Other research suggests that aromatherapy massage may help reduce psychological and endocrine measures of stress in pregnant women and breast cancer patients, and that it may promote immune function in healthy individuals [3-5].
We propose that massage-like techniques involving the topical application of EOs might have positive effects on autonomic balance and immune function in healthy individuals, both immediately and over an extended period of time. In this study, we evaluate the dōTERRA AromaTouch Technique® [ATT] specifically. The ATT is a method of applying EOs by physical touch similar to a massage. It was developed by dōTERRA, a private company that sells EOs, to promote relaxation, stress relief, immune function, and overall wellbeing. This is the first study to examine the benefits of the ATT. To our knowledge, this is also the first study to investigate the benefits of regularly receiving aromatherapy massage for an extended period of time in healthy volunteers.
The outcome measures in this study are associated with different measures of health and wellness, such as autonomic function and endocrine markers of stress, immune secretions, inflammatory biosignals, and psychological anxiety. Cortisol, for instance, is easily measurable in several different body fluids as a parameter of acute, chronic, and diurnal stress levels [6]. High levels of salivary cortisol have been shown to be associated with emotional stress and are believed to be a part of the mechanism linking chronic stress and infection risk [7]. The ease of collecting salivary cortisol has made it a novel alternative to more complex stress biomarker assessments [8,9]. Salivary cortisol levels are unaffected by salivary flow rate or salivary enzymes, and several studies consistently report high correlations between serum and saliva cortisol, indicating that salivary cortisol levels reliably estimate serum cortisol levels [10-13]. Several previous studies have investigated the influence of EO inhalation on salivary cortisol levels, with generally positive results [14-17]. If these effects are from pharmacology (rather than just psychology of aroma sensation) the topical application of oils should have similar (or more pronounced) benefits. Cortisol levels are also reduced by the pressure receptor stimulation induced by massage so the combination of aromatherapy and massage should theoretically have additive effects on reduction of cortisol levels [18].
The salivary glands and their immune secretions are also under autonomic control. Chronic activation of stress pathways decreases salivary secretion of IgA, an antibody protein commonly recognized as the immune system’s initial defense mechanism against microbial colonization [19]. IgA is particularly key in warding off bacterial and viral infections, and it is not only secreted in the saliva, but also in the tears and in the mucous membranes of the respiratory and digestive tracts [19,20]. Studies have shown that aromatherapy massage can promote other measures of immune function, such as serum antibody levels, lymphocyte levels, and a reduction in salivary cortisol levels [3,21,22]. Congruent with these results is the hypothesis that aromatherapy massage may have positive effects on salivary secretory immunoglobulin A [sIgA] levels. BP and HR are also regulated by the ANS, and when elevated they are associated with many disorders and conditions related to stress [23-30]. We expect that aromatherapy massage will have inhibitory effects on these parameters.
Commonly used to assess inflammation in the body, CRP is a positive acute-phase protein; high levels in serum are indicative of inflammation in the body. Although the relationship between salivary and serum CRP levels is not fully understood, salivary CRP is considered an accurate predictor of serum CRP levels symptomatic of systemic inflammation [31]. Results from human and animal research suggest that treatment with EOs may be associated with decreased levels of CRP [32,33].
The four cytokines chosen for analysis in this study were tumor necrosis factor α (TNF-α), interleukin 6 (IL-6), interleukin 1β (IL-1β) , and interleukin 8 (IL-8, which are all common markers of inflammation. Generally, cytokines are known for their salivary levels to correlate reasonably well with serum levels [34,35]. A great deal of research suggests that EOs have potent anti-inflammatory properties, and many EOs and their chemical constituents have been specifically documented for their ability to inhibit inflammatory cytokine production [36-38]. Among the EOs with cytokineinhibitory properties are melaleuca oil and its constituents terpinene-4-ol and α-terpineol, lavender oil, and orange oil’s primary constituent limonene, which are all applied topically to AromaTouch Technique recipients [38-41].
Materials and Methods
Study design
This pilot study used a randomized, single blind, placebocontrolled design. One-half of the subjects were given the ATT with EOs while the other half were given the ATT with the fractionated coconut oil [FCO] placebo. Participants were not informed about which treatment was being received. Participants were treated twice per week for three weeks, with at least two days but no more than four days between each treatment. A total of six treatments were delivered. Data was collected within 5 minutes of treatment completion after the first ATT to evaluate the immediate effects of the technique, and then exactly 24 hours after the final ATT to evaluate lasting effects. A schematic diagram of the experimental design is shown in Figure 1.
Participants
Participants were selected from a group of employees who volunteered to participate in the study. An online screening tool was used to screen potential subjects to ensure their compliance with the study criteria. To decrease the risk of subjects experiencing negative skin reactions, all subjects were required to be between 25-50 years of age, already acquainted with EOs, and self-reported as never having experienced an allergic skin reaction to EOs. To prevent interference with the results, individuals who anticipated life events that might possibly affect the variables measured in this study during the 1 month period of evaluation were excluded from the study. Individuals taking prescription or over-the-counter drugs were also excluded from the study. The subjects’ names were written on paper, drawn at random, and placed into two groups representing the treatment and placebo groups.
For a washout period of one week prior to the study and then for the remainder of the study, subjects refrained from taking any medications, using any EOs, or any EO-containing products. Subjects were advised to avoid strenuous exercise, alcohol, tobacco, over-the-counter medications, and certain foods and drinks before saliva sampling according to the instructions provided by the saliva collection kit manufacturer (Salimetrics, State College, PA).
One subject in the intervention group dropped out of the study prior to its completion because she did not wish to refrain from using other EO products any longer. Her data was still used to evaluate the short-term benefits of the ATT. Thus n=9 for all data for all groups except in the long-term data for the EO group, which was reduced to n=8.
The AromaTouch Technique®
The AromaTouch Technique is an EO application method involving physical touch similar to a massage. The individual administering the ATT applies 3-5 drops (0.15-0.25 mL) of an EO directly to the spine and then rubs the oil into the skin on the back of the recipient. Sometimes the oil is applied to the hands of the administrator and then rubbed on the soles of the feet of the recipient rather than the back. This process is repeated once for eight specific oils and oil blends. Note that the oils and blends used in this technique are known to be safe for topical use, and have been recommended as safe for topical use by dōTERRA’s product safety department. Topical application of these oils is thought to increase the magnitude of benefit by direct absorption into the skin. The oils and blends used in the technique and their primary chemical components, determined by gas chromatography, are given below:
1. dōTERRA Balance® blend: linalool (30%), bornyl ace tate(19%), α-pinene (16%)
2. Lavender EO: linalool (30%), linalyl acetate (37%)
3. Melaleuca EO: terpinen-4-ol (43%), γ-terpinene (19%)
4. dōTERRA On Guard® blend: limonene (44%), eugenol (36%)
5. dōTERRA AromaTouch® blend: menthol (14%), lina lool(13%), limonene (12%), α- pinene (11%)
6. dōTERRA Deep Blue® blend: methyl salicylate (32%),menthol (12%)
7. Wild orange EO: limonene (95%)
8. Peppermint EO: menthone (36%), menthol (30%)
2. Lavender EO: linalool (30%), linalyl acetate (37%)
3. Melaleuca EO: terpinen-4-ol (43%), γ-terpinene (19%)
4. dōTERRA On Guard® blend: limonene (44%), eugenol (36%)
5. dōTERRA AromaTouch® blend: menthol (14%), lina lool(13%), limonene (12%), α- pinene (11%)
6. dōTERRA Deep Blue® blend: methyl salicylate (32%),menthol (12%)
7. Wild orange EO: limonene (95%)
8. Peppermint EO: menthone (36%), menthol (30%)
The total amount of EO applied to the skin during this procedure is 24-40 drops (1.2-2.0 mL), since 3-5 drops (0.15-0.25 mL) are used for each of the eight EOs in the technique. The full ATT usually lasts about 45 minutes. The method of administration of this technique for controls was completely identical to the process outlined above, except with FCO replacing each EO.
Testing procedures
All measurements including cardiovascular parameters, anxiety inventory, and saliva samples were taken before the first ATT for each participant. These measurements were then repeated immediately after its completion. A final round of measurements was taken exactly 24 hours after the final ATT. Note that the final measurements were taken at the exact same time of day as the first set of measurements, controlling for diurnal cortisol fluctuation.
Because subjects were lying face down during the entire ATT, they were quite literally blind to their surroundings. However, to prevent subjects from using their sense of smell to determine which group they had been placed in, the administration room was intentionally filled with the scent of EOs during each step of the technique. The administrator accomplished this by placing a drop of EO on the floor rather than on the back or feet of the recipient just before applying the FCO. The administrator also used other techniques, such as setting down different bottles at different times to reinforce the illusion that they were using different EOs rather than the coconut oil placebo. This was done to replicate the sounds and smells that would be experienced if the individuals were receiving the technique with EOs.
For both groups, the technique was given in the same room which had dimensions 10 ftx12 ftx10 ft. The same music was played during every session for members of both groups. The music was of the spa style and can be accessed at the following URL: https://www.youtube. com/watch?v=VP-5GNJSw4g.
The lights in the room were dimmed to the same brightness, and the same two therapists delivered the technique. Recipients received their techniques from one of two trained therapists on the first session of the week, and then from the other therapist on the second session of the week.
Cardiovascular measurements
Systolic [SYS] and diastolic [DIA] blood pressure [BP] and heart rate [HR] were measured using the Omron 10 model BP786N digital cuff. The cuff was used on the left arm for all participants. Data was recorded using the average of three consecutive measurements. Mean Arterial Pressure [MAP] was calculated according to the formula MAP =[(2xDIA)+SYS]/3.
Saliva biomarker analysis
Whole saliva samples were collected with Saliva Bio’s 2 mL cryovials and the Saliva Collection Aid (exclusively from Salimetrics, State College, PA), a collection device specifically designed to improve volume collection and increase participant compliance, and validated for use with all analytes used in this study. Drool time and sample volume were recorded immediately after sample collection. Samples were promptly placed on dry ice and placed in storage at -20 °C. After all samples had been collected, they were shipped overnight on dry ice to SalivaBio Lab (Carlsbad, CA, USA) for analysis. All samples were tested for cortisol, secretory immunoglobulin A [sIgA], C-reactive protein [CRP], and a panel of four cytokines: IL-1β, IL-6, IL-8, and TNF-α.
Spielberger state anxiety inventory
Anxiety scores were evaluated using the Spielberger State-Trait Anxiety Inventory. Only the state anxiety questions were used in this study; trait anxiety questions were omitted. The Spielberger State Anxiety Inventory [SSAI] questions were incorporated into an online questionnaire that subjects completed using a tablet device.
Statistical analysis
Differences between groups after treatment were analyzed using one-way ANCOVA, which bears the most statistical power in direct comparison to other clinically relevant statistical methods [42]. Adjusted means were obtained using baseline data as the concomitant (covariate) variable. Statistical significance of the differences between group means after treatment w as determined using the F-test. Confidence intervals w ere computed using the mean-square error for dataset. The analysis w as performed using the computational tool “One-Way ANCOVA for 2 Independent Samples” provided by Vassar Stats, a free web-based statistical computation service.
Results
Immediate effects of the technique
The effect of the ATT with EOs was clearly different from the ATT with FCO alone, and many of the differences were statistically significant, although difficult to generalize due to the small sample size (Table 1). After adjusting for baseline differences, subjects given the ATT with EOs experienced a -12.2% decrease in HR of -8.9±1.44 beats/minute) on average after the ATT, compared to controls treated with coconut oil only whose HR decreased by only about -2.5% (about -1.8±1.44 beats/minute) on average. The difference in percent decrease between groups was markedly statistically significant, with a p-value of 0.0002. SYS BP, DIA BP, and MAP each decreased slightly in the EO group but increased slightly in the FCO placebo group after the A TT. None of these measures achieved statistical significance.
Cortisol levels decreased about -26.8% (-68±46 ng/dL) on average following the ATT with EOs, but only decreased by -21.7% (-55±46 ng/dL) in the placebo group, although the difference was not statistically significant. Salivary CRP was also lower in the group treated with EOs, with a decrease of -32.9% (-5.45±3.3 ng/mL) that was statistically significant, with a p-value of 0.048 (Table 1). No meaningful differences in salivary sIgA secretion or cytokine levels were observed between groups immediately after the first session.
Scores on the SSAI also decreased in both groups after the ATT. Subjects in the EO group experienced a percent change of -33.8% (-13.21±2.06 points), on average, while subjects in the FCO group experienced a percent change of only -24.3% (-9.51±2.06 points). This difference between groups did not reach statistical significance.
Lasting effects from regularly receiving the technique
The quantitative differences in the various inflammatory biomarkers between the intervention and placebo groups were pronounced (Table 2). Three of the four cytokine levels measured, TNF-α, IL-1β, and IL-8, showed remarkable decrease in the ATT with EOs group, with percent changes of -64.4%, -63.5%, and -59.7%, respectively. The differences between the EOs and FCO groups’ average levels of these cytokines 24 hours after the final treatment achieved statistical significance, with p-values of 0.005, 0.006, and 0.001, respectively. The difference in salivary IL-6 was a noteworthy -73.1% which approached statistical significance with a p-value of 0.07. The difference in salivary CRP between groups was also marked and significant. Subjects in the EO group exhibited a -71.1% decrease in CRP levels, while CRP levels of those in the FCO group actually increased by a negligible amount. Again, the difference between groups reached statistical significance, with a p-value of 0.05. These results suggest a lasting beneficial impact of the ATT on inflammation, as demonstrated by the statistically significant difference between groups in four of the five measured inflammatory biosignals. The ATT with EOs group showed an overall decrease in HR, MAP, DIA BP, and SYS BP, while the ATT with FCO showing a decrease in only MAP, DIA BP, and SYS BP. Indeed, the ATT and FCO group actually saw an increase in HR (Table 2). While the decrease in these parameters was more pronounced in the treatment group, the difference between groups did not achieve statistical significance.
In both groups, scores on the SSAI once again decreased. Subjects in the intervention group experienced a percent change of -27.6±3.14, whereas the control group experienced a point change of -19.7±3.14, a difference that was not statistically significant (Table 2). However, this assessment would likely achieve statistical significance with a larger sample size. We did not observe any significant differences in sIgA secretion or cortisol levels between groups or compared to baseline after the three weeks.
Discussion
Our results in healthy volunteers suggest that aromatherapy massage and techniques like the ATT should be investigated for their potential to help reduce HR, BP, and MAP in individuals with acute or chronic anxiety. The menthol content in peppermint oil, Deep Blue® blend, and the AromaTouch® blend may explain these effects, at least in part. Menthol has been identified as a calcium channel blocker that acts on both smooth and cardiac muscle [43,44]. Its action on L-type calcium channels suggests the same mechanism as the calcium channel blocker nifedipine, which is used clinically to reduce heart rate and blood pressure [43,44].
Although a subjective measure, the psychological perception of stress or relaxation is an important outcome of the ATT from a patient’s perspective. We found that perceived anxiety decreased considerably after receiving the ATT with EOs and was significantly greater than the decrease in anxiety experienced by individuals receiving the touch procedure with the inactive FCO. The pharmacology of certain EO constituent compounds may be linked with these effects. Lavender oil is known to block N-type, P/Q-type, and T-type voltage-dependent calcium channels similarly to the anxiolytic drug pregabalin, and it has been recommended for clinical use in patients suffering from anxiety [45]. Its constituents linalool and linalyl acetate are also known for their ability to potentiate GABAA currents in electrophysiology experiments and have demonstrated anxiolytic and sedative effects in animal models [46,47]. The main compound in melaleuca oil, terpinene-4-ol, also potentiates GABAergic neurotransmission and may have similar effects [48]. α-pinene, found in both the Balance® and AromaTouch® blends, is a partial GABAA agonist with direct interaction at the benzodiazepine site [49]. Bornyl acetate, a compound found in the AromaTouch blend, is also documented for anxiolytic effects, which are described as being specifically mediated by altering autonomic nervous system activity [50].
Perhaps the most significant finding in this study was the lasting effects of the EOs on inflammatory biomarkers. CRP and cytokine levels were significantly reduced in the EOs group but not the FCO group, suggesting that the effects were due to the activity of the EOs specifically and not the touch procedure. Furthermore, the reduction in these biomarkers was considerable. Each was reduced two- to three-fold compared to either baseline or FCO controls. These results suggest that regular topical application of EOs in a massage-like touch procedure may bear considerable implications for patients with inflammatory disorders.
Conclusion
It is well-known that the moderate pressure touch associated with massage can have positive effects on anxiety and stress. The current study design made it possible to control for the effects of the touch procedure and determine the extent to which the EOs affected patients receiving the ATT. The EOs used in the ATT robustly enhanced the relaxing effects of the touch procedure as measured immediately after the technique’s administration. Our findings suggest that the ATT, which employs both physical touch and EOs, should be considered for practitioners or patients seeking to manage acute stress or anxiety as a complementary or alternative therapy.
Our data also suggests that the EOs are responsible for additional benefits not associated with the touch procedure. Regular administration of the technique with EOs may have positive effects on systemic inflammation by reducing endogenous inflammatory signals. Future research in patients with inflammatory disorders should be conducted to further explore the benefits of the ATT with EOs in this context.
Acknowledgements
This study was funded by dōTERRA Intl. (Pleasant Grove, UT, USA) and the saliva analysis was conducted at SalivaBio Lab (Carlsbad, CA, USA). Questionnaires and surveys were built and administered by SurveyMonkey. com, a paid web survey service. T. Bahr interpreted the data, performed the statistical analysis, and wrote the paper. D. Rodriguez and K. Allred participated in the writing of the paper. We acknowledge Jordan Hanks, Shane Beck, Alex Agle, Hillary Slaughter, and Emily Miller for their help in collecting data and/or administering the AromaTouch Techniques. We also acknowledge Baylee Van Camp and Lindsey Humes for assisting with scheduling and correspondence.
References
- Hongratanaworakit T (2010) Stimulating effect of aromatherapy massage with jasmine oil. Nat Prod Commun 5: 157-162.
- Chuang KJ, Chen HW, Liu IJ, Chuang HC, Lin LY (2014) The effect of essential oil on heart rate and blood pressure among solus por aqua workers. Eur J Prev Cardiol 21: 823-828.
- Chen PJ, Chou CC, Yang L, Tsai YL, Chang YC, et al. (2017) Effects of aromatherapy massage on pregnant women's stress and immune function: a longitudinal, prospective, randomized controlled trial. J Altern Complement Med 23: 778-786.
- Imanishi J, Kuriyama H, Shigemori I, Watanabe S, Aihara Y, et al. (2009) Anxiolytic effect of aromatherapy massage in patients with breast cancer. Evid Based Complement Alternat Med 6: 123-128.
- Kuriyama H, Watanabe S, Nakaya T, Shigemori I, Kita M, et al (2005) Immunological and psychological benefits of aromatherapy massage. Evid Based Complement Alternat Med 2: 179-184.
- Miller WL (2008) Steroidogenic enzymes. Endocr Dev 13: 1-18.
- Oikawa J, Ukawa S, Ohira H, Kawamura T, Wakai K, et al. (2015) Diabetes mellitus is associated with low secretion rates of immunoglobulin a in saliva. J Epidemiol 25: 470-474.
- Bozovic D, Racic M, Ivkovic N (2013) Salivary cortisol levels as a biological marker of stress reaction. Med Arch 67: 374-377.
- Hodgson NA, Granger DA (2013) Collecting saliva and measuring salivary cortisol and alpha-amylase in frail community residing older adults via family caregivers. J Vis Exp: e50815.
- Vining RF, McGinley RA (1987) The measurement of hormones in saliva: possibilities and pitfalls. J Steroid Biochem 27: 81-94.
- Francis SJ, Walker RF, Riad-Fahmy D, Hughes D, Murphy JF, et al. (1987) Assessment of adrenocortical activity in term newborn infants using salivary cortisol determinations. J Pediatr 111: 129-133.
- Hiramatsu R (1981) Direct assay of cortisol in human saliva by solid phase radioimmunoassay and its clinical applications. Clin Chim Acta 117: 239-249.
- Vining RF, McGinley RA, Maksvytis JJ, Ho KY (1983) Salivary cortisol: a better measure of adrenal cortical function than serum cortisol. Ann Clin Biochem 20: 329-335.
- Kim IH, Kim C, Seong K, Hur MH, Lim HM, et al (2012) Essential oil inhalation on blood pressure and salivary cortisol levels in prehypertensive and hypertensive subjects. Evid Based Complement Alternat Med 2012: 984203.
- Jafarzadeh M, Arman S, Pour FF (2013) Effect of aromatherapy with orange essential oil on salivary cortisol and pulse rate in children during dental treatment: a randomized controlled clinical trial. Adv Biomed Res 2: 10.
- Atsumi T, Tonosaki K (2007) Smelling lavender and rosemary increases free radical scavenging activity and decreases cortisol level in saliva. Psychiatry Res 150: 89-96.
- Toda M, Morimoto K (2008) Effect of lavender aroma on salivary endocrinological stress markers. Arch Oral Biol 53: 964-968.
- Field T (2016) Massage therapy research review. Complement Ther Clin Pract 24: 19-31.
- Tsujita S, Morimoto K (1999) Secretory IgA in saliva can be a useful stress marker. Environ Health Prev Med 4: 1-8.
- Trochimiak T, Hübner-Woźniak E (2012) Effect of exercise on the level of immunoglobulin a in saliva. Biol Sport 29: 255-261.
- Wu JJ, Cui Y, Yang YS, Kang MS. Jung SC, et al. (2014) Modulatory effects of aromatherapy massage intervention on electroencephalogram, psychological assessments, salivary cortisol and plasma brain-derived neurotrophic factor. Complement Ther Med 22: 456-462.
- Khiewkhern S, Promthet S, Sukprasert A, Eunhpinitpong W, Bradshaw P (2013) Effectiveness of aromatherapy with light thai massage for cellular immunity improvement in colorectal cancer patients receiving chemotherapy. Asian Pac J Cancer Prev 14: 3903-3907.
- Licht CM, de geus EJ, van dyck R, Penninx BW (2009) Association between anxiety disorders and heart rate variability in the Netherlands Study of Depression and Anxiety (NESDA). Psychosom Med 71: 508-518.
- Pan Y, Cai W, Cheng Q, Dong W, An T, et al. (2015) Association between anxiety and hypertension: a systematic review and meta-analysis of epidemiological studies. Neuropsychiatr Dis Treat 11: 1121-1130.
- Stein DJ, Aguilar-gaxiola S, Alonso J, Bruffaerts R, de Jonge P, et al. (2014) Associations between mental disorders and subsequent onset of hypertension. Gen Hosp Psychiatry 36: 142-149.
- Ginty AT, Carroll D, Roseboom TJ, Phillips AC, de Rooij SR (2013) Depression and anxiety are associated with a diagnosis of hypertension 5 years later in a cohort of late middle-aged men and women. J Hum Hypertens 27: 187-190.
- Grimsrud A, Stein DJ, Seedat S, Williams D, Myer L (2009) The association between hypertension and depression and anxiety disorders: results from a nationally-representative sample of South African adults. PLoS ONE 4: e5552.
- Shinn EH, Poston WS, Kimball KT, St Jeor ST, Foreyt JP (2001) Blood pressure and symptoms of depression and anxiety: a prospective study. Am J Hypertens 14: 660-664.
- Thayer JF, Lane RD (2007) The role of vagal function in the risk for cardiovascular disease and mortality. Biol Psychol 74: 224-242.
- Friedman BH (2007) An autonomic flexibility-neurovisceral integration model of anxiety and cardiac vagal tone. Biol Psychol 74: 185-199.
- Ouellet-morin I, Danese A, Williams B, Arseneault L (2011) Validation of a high-sensitivity assay for C-reactive protein in human saliva. Brain Behav Immun 25: 640-646.
- Duijker G, Bertsias A, Symvoulakis EK, Moschandreas J, Malliaraki N, et al. (2015) Reporting effectiveness of an extract of three traditional Cretan herbs on upper respiratory tract infection: results from a double-blind randomized controlled trial. J Ethnopharmacol 163: 157-166.
- Liu Y, Iwasaki T, Watarai S, Kodama H (2004) Effect of turpentine oil on C-reactive protein (CRP) production in rainbow trout (Oncorhynchus mykiss). Fish Shellfish Immunol 17: 203-210.
- Fernandez-Botran R, Miller JJ, Burns VE, Newton TL (2011) Correlations among inflammatory markers in plasma, saliva and oral mucosal transudate in post-menopausal women with past intimate partner violence. Brain Behav Immun 25: 314-321.
- La fratta I, Tatangelo R, Campagna G, Rizzuto A, Franceschelli S, et al. (2018) The plasmatic and salivary levels of IL-1β, IL-18 and IL-6 are associated to emotional difference during stress in young male. Sci Rep 8: 3031.
- de cássia da Silveira E Sá R, Andrade LN, Dos Reis Barreto de Oliveira R, de Sousa DP (2014) A review on anti-inflammatory activity of phenylpropanoids found in essential oils. Molecules 19: 1459-1480.
- Tsai ML, Lin CC, Lin WC, Yang CH (2011) Antimicrobial, antioxidant, and anti-inflammatory activities of essential oils from five selected herbs. Biosci Biotechnol Biochem 75: 1977-1983.
- Taga I, Lan CQ, Altosaar I (2012) Plant essential oils and mastitis disease: their potential inhibitory effects on pro-inflammatory cytokine production in response to bacteria related inflammation. Nat Prod Commun 7: 675-682.
- Nogueira MN, Aquino SG, Rossa Junior C, Spolidorio DM (2014) Terpinen-4-ol and alpha-terpineol (tea tree oil components) inhibit the production of IL-1β, IL-6 and IL-10 on human macrophages. Inflamm Res 63: 769-778.
- Ueno-Iio T, Shibakura M, Yokota K, Aoe M, Hyoda T, et al. (2014) Lavender essential oil inhalation suppresses allergic airway inflammation and mucous cell hyperplasia in a murine model of asthma. Life Sci 108: 109-115.
- Yoon WJ, Lee NH, Hyun CG (2010) Limonene suppresses lipopolysaccharide-induced production of nitric oxide, prostaglandin E2, and pro-inflammatory cytokines in RAW 264.7 macrophages. J Oleo Sci 59: 415-421.
- Vickers AJ (2001) The use of percentage change from baseline as an outcome measure in a controlled trial is statistically inefficient: a simulation study. BMC Med Res Methodol 1: 6.
- Amato A, Liotta R, Mulè F (2014) Effects of menthol on circular smooth muscle of human colon: analysis of the mechanism of action. Eur J Pharmacol 740: 295-301.
- Baylie RL, Cheng H, Langton PD, James AF (2010) Inhibition of the cardiac L-type calcium channel current by the TRPM8 agonist, (-)-menthol. J Physiol Pharmacol 61: 543-550.
- Schuwald AM, Nöldner M, Wilmes T, Klugbauer N, Leuner K, et al. (2013) Lavender oil-potent anxiolytic properties via modulating voltage dependent calcium channels. PLoS ONE 8: e59998.
- Milanos S, Elsharif SA, Janzen D, Buettner A, Villmann C (2017) Metabolic products of linalool and modulation of GABAA Receptors. Front Chem 5: 46.
- Takahashi M, Satou T, Ohashi M, Hayashi S, Sadamoto K, et al. (2011) Interspecies comparison of chemical composition and anxiolytic-like effects of lavender oils upon inhalation. Nat Prod Commun 6: 1769-1774.
- Nóbrega FF, Salvadori MG, Masson CJ, Mello CF, Nascimento TS, et al. (2014) Monoterpenoid terpinen-4-ol exhibits anticonvulsant activity in behavioural and electrophysiological studies. Oxid Med Cell Longev 2014: 703848.
- Yang H, Woo J, Pae AN, Um MY, Cho NC, et al. (2016) α-Pinene, a major constituent of pine tree oils, enhances non-rapid eye movement sleep in mice through GABAA-benzodiazepine receptors. Mol Pharmacol 90: 530-539.
- Matsubara E, Fukagawa M, Okamoto T, Ohnuki K, Shimizu K, et al. (2011) (-)-Bornyl acetate induces autonomic relaxation and reduces arousal level after visual display terminal work without any influences of task performance in low-dose condition. Biomed Res 32: 151-157.