
Journal of Orthopedics & Rheumatology
Download PDF
Case Report
*Address for Correspondence: Kazutoshi Hamada, MD, PhD, Department of Orthopaedics, Machida-keisen Hospital, 1546-2, Ogawa, Machida City, Tokyo 194-0003, Japan, Tel: +81-42-795-1668; Fax: +81-42-795-6217; E-mail: kazuhama@muj.biglobe.ne.jp
Citation: Hamada K, Yamanaka K, Ueno M, Mikasa T, Uchiyama Y. Presumed Primary Frozen Shoulder - Clinical Characteristics and Findings of Magnetic Resonance Imaging. J Orthopedics Rheumatol. 2015; 2(1): 4.
Copyright © 2015 Hamada K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Orthopedics & Rheumatology | ISSN: 2334-2846 | Volume: 2, Issue: 1
Submission: 23 November 2015 | Accepted: 16 December 2015 | Published: 21 December 2015
Keywords: Frozen shoulder; Stiff shoulder; Shoulder impingementsyndrome; Bursitis; Rotator cuff tear; Magnetic resonance imaging
Abbreviation: MRI: Magnetic Resonance Imaging; Th: Thoracic spine spinous process; L: Lumbar spine spinous process; ROM: Range of Motion; Flex: Flexion; ER: External Rotation; IR: Internal Rotation at side; SAB: Subacromial Bursa; GHJ: Glenohumeral Joint; BG: Sheath of Bicipital Groove; ACJ: Acromioclavicular Joint; ROC curve: Receiver Operating Characteristic curve; AUC: Area Under the Curve
Signal intensities in the cuff tendons and fluid collection in the cavities were independently estimated by three orthopedic surgeons (K.H., K.Y., T.M.), and the diagnosis was subsequently established by consensus when the surgeons’ interpretations of MRI findings differed.
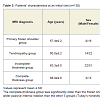
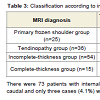
Passive flexion, passive external rotation, and duration of disease at an initial visit did not show significant differences among four groups. However, the complete-thickness group was significantly older than the the primary frozen shoulder group (p=0.01) and the tendinopathy group (p=0.08), but was not significantly different from the incomplete-thickness group (p=0.157) (Tukey’s honestly significant difference test). The complete-thickness group also showed significantly wider passive internal rotation than the other three groups (Tukey’s honestly significant difference test, p=0.00, 0.005, 0.003, respectively). In the passive internal rotation analysis, the area under the curve of the receiver operating characteristic curve was 0.752 and operating characteristic was good (95% confidence interval, 0.595-0.910). The cutoff value offering the highest value for (sensitivity - false-positive rate) was Th16.5 (L4.5). If Th16.5 (L4.5) was set as cutoff value, sensitivity was 0.561, and the false-positive rate was 0.143 for the complete-thickness group (Figure 1 ). There were 73 patients with internal rotation restriction of Th17 (L5) or more caudal and only three cases (4.1%) were in the complete-thickness group (Table 3).<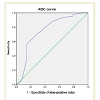
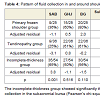
Patterns of fluid collection in the cavities are shown in Table 4. The incomplete-thickness group showed significantly the most frequent fluid collection in the subacromial bursa, and the tendinopathy group showed the least frequent (Pearson’s chi-square test, p=0.001). Other forms of fluid collections did not differ significantly among these three groups.
Presumed Primary Frozen Shoulder - Clinical Characteristics and Findings of Magnetic Resonance Imaging
Kazutoshi Hamada1*, Kaoru Yamanaka2, JohannesMenzel2, Masaki Ueno1, Takahiko Mikasa3 and Yoshiyasu Uchiyama4
- 1Department of Orthopaedics, Machida-keisen Hospital, Ogawa, Machida City, Tokyo, Japan
- 2Yamanaka Orthopaedic Clinic, Shizuoka City, Shizuoka, Japan
- 3Shinyokohama Orthopaedics /Rheumatology, Yokohama City, Kanagawa, Japan
- 4Department of Orthopedics, Tokai University Hospital, Isehara City, Kanagawa, Japan
*Address for Correspondence: Kazutoshi Hamada, MD, PhD, Department of Orthopaedics, Machida-keisen Hospital, 1546-2, Ogawa, Machida City, Tokyo 194-0003, Japan, Tel: +81-42-795-1668; Fax: +81-42-795-6217; E-mail: kazuhama@muj.biglobe.ne.jp
Citation: Hamada K, Yamanaka K, Ueno M, Mikasa T, Uchiyama Y. Presumed Primary Frozen Shoulder - Clinical Characteristics and Findings of Magnetic Resonance Imaging. J Orthopedics Rheumatol. 2015; 2(1): 4.
Copyright © 2015 Hamada K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Orthopedics & Rheumatology | ISSN: 2334-2846 | Volume: 2, Issue: 1
Submission: 23 November 2015 | Accepted: 16 December 2015 | Published: 21 December 2015
Abstract
Purpose: To determine rotator cuff pathologies in patients with painful and stiff shoulder using plain magnetic resonance imaging, and to assess differences in patients’ characteristics and patterns of fluid collection in and around the shoulder joint.Methods: Magnetic resonance imaging studies were performed on 130 shoulders of 126 patients who were 40 years or older with passive flexion 120 degrees or less, and no history of trauma. The patients’ characteristics at the initial visit, the supraspinatus tendon insertion and fluid collection in and around the shoulder joint were studied.
Results: Patients were diagnosed as showing complete-thickness tear (n=15, 12%), incomplete-thickness tear (n=54, 42%), tendinopathy (n=36, 27%), or primary frozen shoulder (n=25, 19%). Age at an initial visit was significantly older in the complete-thickness group than in the other two groups. The complete-thickness group showed significantly wider passive internal rotation than the other two groups, and could be differentiated with a probability of 96%, if the internal rotation restriction was set at L5 or more caudal. The incomplete-thickness group showed fluid collection in the subacromial bursa significantly more frequently than the primary frozen shoulder group.
Conclusion: Almost all patients with stiff shoulder had minor cuff pathologies or frozen shoulder, if the internal rotation restriction wassevere.
Keywords: Frozen shoulder; Stiff shoulder; Shoulder impingementsyndrome; Bursitis; Rotator cuff tear; Magnetic resonance imaging
Abbreviation: MRI: Magnetic Resonance Imaging; Th: Thoracic spine spinous process; L: Lumbar spine spinous process; ROM: Range of Motion; Flex: Flexion; ER: External Rotation; IR: Internal Rotation at side; SAB: Subacromial Bursa; GHJ: Glenohumeral Joint; BG: Sheath of Bicipital Groove; ACJ: Acromioclavicular Joint; ROC curve: Receiver Operating Characteristic curve; AUC: Area Under the Curve
Introduction
The clinical presentation of frozen shoulder (adhesive capsulitis) is nonspecific and consists of limited passive motion accompanied by pain. The current consensus definition of frozen shoulder by the American Shoulder and Elbow Surgeons is “a condition of uncertain etiology characterized by significant restriction of both active and passive shoulder motion that occurs in the absence of a known intrinsic shoulder disorder” [1,2]. Calcific tendinitis, bicipital tenosynovitis, glenohumeral and acromioclavicular arthritis, and rotator cuff tears should be excluded when diagnosing primary frozen shoulder [3]. In 1991, Wiley reported that only 37 patients (24.7%) qualified for diagnosis of primary frozen shoulder out of 150 patients clinically diagnosed with frozen shoulder [4]. The others had frozen shoulder secondary to some other painful cause, such as rotator cuff tear or impingement. In 2011, Zuckerman and Rokito reported the present consensus definition of frozen shoulder to the membership of the American Shoulder and Elbow Surgeons [5]. MRI characteristics for the diagnosis of frozen shoulder have been reported using contrast or plain MRI [6-10]. Several reports have described diagnosis using MRI findings for painful and stiff shoulders from a converse direction [7,11,12]. The purpose of this study was to disclose the different patterns of clinical findings and fluid collection in and around the shoulder joint, as well as to determine the rotator cuff pathologies present in patients with painful and stiff shoulders using plain MRI.Materials and Methods
Patients and/or their families were informed that data from the case would be submitted for publication, and provided consent prior to enrolment. Approval was given by the institutional review board at the hospitals.Plain MRI studies were performed on consecutive 192 shoulders of 185 patients with persistent shoulder pain. Of these 185 patients, 130 shoulders of 126 patients (44 men, 82 women) who showed passive flexion ≤120 degrees with recognizable restriction in the ranges of external and internal rotation, age ≥40 years, and history of symptoms continuing for more than one month were enrolled in the study. The mean age of patients at initial examination was 62.1 years (range, 42-82 years). The right shoulder was involved in 63 patients, the left in 59, and four showed bilateral shoulder involvement. The exclusion criteria were: a history of trauma in or around the shoulder joint, such as a fracture; presence of calcium deposits in or around shoulder joint on radiography; osteoarthritis of the shoulder; rheumatoid arthritis; cervical spine disease, dialysis; or nerve palsy. No patients had received any injections into the shoulder joint or subacromial bursa three months prior to MRI.
MRI was performed using a 1.5-T system (Signa Horizon LX, GE Healthcare, Milwaukee, WI) using a shoulder coil. T2-weighted fast spin-echo inversion recovery (FSEIR) images [repetition time, 4200 ms; echo time, 80 ms; inversion time, 150 ms; matrix, 256 × 192; slice thickness, four mm (slice interval, 0.4 mm), field of view, 17 × 17 cm] were obtained in the coronal oblique and transverse planes. Thickness of the axillary capsule could not be estimated precisely, but examinations of all shoulders revealed thickening of the axillary capsule and synovia [13].
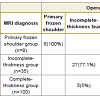
Complete- and incomplete-thickness rotator cuff tears were diagnosed according to the methods described by Teefey et al. [14]. Signal intensities in the supraspinatus tendons, except for in the incomplete-thickness and complete-thickness tears, were classified into three grades: low intensity; scattered muscle-intensity; and scattered fluid-intensity. The group showing low intensity was called the primary frozen shoulder group, and the group showing scattered muscle-intensity or scattered fluid-intensity was called the tendinopathy group [15-17]. As to the diagnostic rate from MRI, the following pilot study was performed. A total of 143 shoulders with subacromial impingement syndrome were operated on after MRI. The aforementioned criteria were applied, and 100 shoulders were diagnosed with complete-thickness tear (completethickness group), 35 shoulders with incomplete-thickness tear of the supraspinatus tendon (incomplete-thickness group), and eight shoulders with primary frozen shoulder (primary frozen shoulder group) preoperatively. The diagnostic rates in our MRI study were 100% for primary frozen shoulder, 77.1% for incomplete-thickness tears, and 95% for complete-thickness tears (Table 1). Fluid collection in the subacromial bursa, glenohumeral joint, bicipital groove, subscapularis bursa, and acromioclavicular joint were estimated as positive if the cavities were distended by fluid-intensity signals [10]. Because the subacromial bursa and glenohumeral joint are connected such that complete-thickness tears make it difficult to estimate fluid in those areas, fluid collection in cavities was estimated in all except for the complete-thickness group.
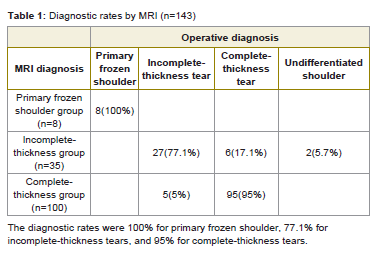
Table 1: Diagnostic rates by MRI (n=143)
Statistical analysis
Differences in patients’ characteristics (age at an initial visit, symptom duration prior to an initial visit, passive range of motion) among the primary frozen shoulder group, tendinopathy group, incomplete-thickness group, and complete-thickness group were determined by one-way analysis of variance and a multiple comparison test (Tukey’s honestly significant difference test) using SPSS II version 17.0 (SPSS, Chicago, IL). Differences in fluid collection rates between groups of patients were evaluated with the chi-square test using SPSS II version 17.0 (SPSS). The level of statistical significance was set at P < 0.05. On passive internal rotation, the receiver operating characteristic curve was described, and cutoff values were analyzed.
Results
From MRI diagnosis, the complete-thickness group comprised 15 shoulders (12%) including one massive tear, the incomplete-thickness group comprised 54 (42%), the tendinopathy group comprised 36 (27%), and the primary frozen shoulder group comprised 25 (19%). Patients’ characteristics at the initial visit are shown in Table 2.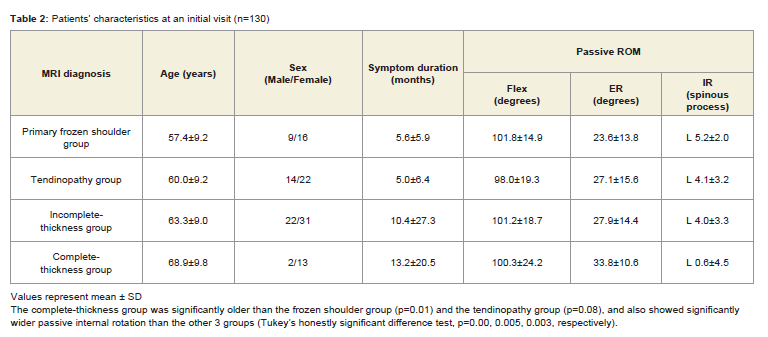
Table 2: Patients’ characteristics at an initial visit (n=130)
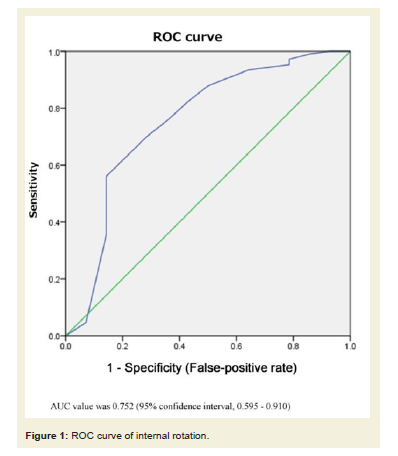
Figure 1: ROC curve of internal rotation.
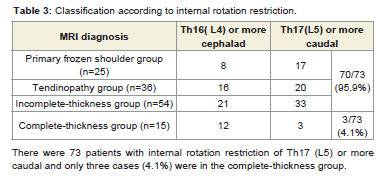
Table 3: Classification according to internal rotation restriction.
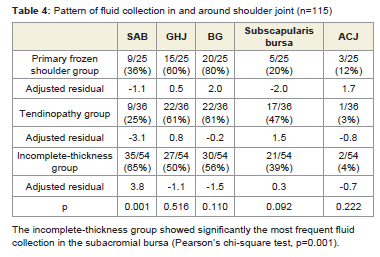
Table 4: Pattern of fluid collection in and around shoulder joint (n=115)
Discussion
In 1992, Shaffer et al. followed-up 68 frozen shoulders after rotator cuff tears had been excluded by arthrography for seven years (mean), and 31 (50%) still experienced pain or stiffness [18]. Connell et al. reported three partial tears of the supraspinatus tendon disclosed by intravenous gadolinium-enhanced MR arthrography in 24 consecutive patients with clinical evidence of adhesive capsulitis [7]. In 2009, Yoo et al. reported that 50 patients (61.7%) in a group believed to have stage-2 idiopathic adhesive capsulitis showed incomplete- or complete-thickness tears on MR arthrography [12]. In our study, plain MRI was applied and, almost half of the shoulders displayed incomplete- or complete-thickness tears, with only 19% displaying primary frozen shoulder. Our report is consistent with previous reports. The report of Shaffer et al. may thus have also included incomplete-thickness tears, which could have made the prognosis for clinically diagnosed frozen shoulder appear worse than expected [18].Yoo et al. also reported that adhesive capsulitis patients >60 years old were more likely to have a supraspinatus tendon tear [12]. Our results were consistent with this finding; mean age of the primary frozen shoulder group was 57.4 ± 9.2 years, compared to 60.0 ± 9.2 years in the tendinopathy group, and these groups were significantly younger than the complete-thickness group (68.9 ± 9.8 years).
In our study, passive flexion and passive external rotation at an initial visit did not show significant differences among four groups, but the range of passive internal rotation of the complete-thickness group was significantly wider than that of the other three groups. This is believed to be a characteristic of complete-thickness tear with a restricted range of motion, due to less shoulder pain in the completethickness tears than the other rotator cuff pathologies [19].
Only three shoulders out of 73 patients with passive internal rotation restriction of L5 or more caudal were in the completethickness group. This means that 95.9 % of patients in whom passive internal rotation restriction was L5 or more caudal were not diagnosed as complete-thickness rotator cuff tear (Table 3), and further imaging studies for complete-thickness tear may not necessary.
In 1997, Tamai et al. reported one shoulder in 6 primary frozen shoulders and four shoulders in 12 tendinopathies displayed fluid collection in the subacromial bursa on the results of dynamic MRI for 18 frozen shoulders [10]. In our study, the incomplete-thickness group showed the most frequent fluid collection in the subacromial bursa. The primary frozen shoulder group and tendinopathy group showed fluid collection in 36% and 25%, respectively, which may be due to synovitis causing restricted shoulder motion [10]. The primary frozen shoulder group showed no significant differences from the tendinopathy group in any parameters.
This study has several limitations. First, not all patients underwent operations and we thus did not have surgical proof of MRI findings. However, according to clinical symptoms and MRI findings, our primary frozen shoulder group was considered compatible with primary frozen shoulder. Second, we were unable to differentiate phases of frozen shoulder, because not all patients could be followedup until clinical remission. Nevertheless, our results disclosed the existence of rotator cuff pathologies and also the different patterns of clinical findings and fluid collection in stiff and painful shoulders. Third, the mechanism of relatively gentle internal rotation restriction in complete-thickness rotator cuff tear was not disclosed exactly in this study. This issue remains to be studied in the future.
In conclusion, almost all patients with stiff shoulder had minor cuff pathologies or frozen shoulder, if the internal rotation restriction
Acknowledgements
We thank the Radiology Service staff at Shizuoka Red Cross Hospital for their cooperation and technical assistance.References
- Hsu JE, Anakwenze OA, Warrender WJ, Abboud JA (2011) Current review of adhesive capsulitis. J Shoulder Elbow Surg 20: 502-514.
- Zuckerman JD, Cuomo F (1993) Frozen shoulder-A balance of mobility and stability. In: The shoulder, American Academy of Orthopaedic Surgeons, Chicago.
- Neviaser RJ (1983) Painful conditions affecting the shoulder. Clin Orthop Relat Res 173: 63-69.<
- Wiley AM (1991) Arthroscopic appearance of frozen shoulder. Arthroscopy 7: 138-143.
- Zuckerman JD, Rokito A (2011) Frozen shoulder: a consensus definition. J Shoulder Elbow Surg 20: 322-325.
- Carrillon Y, Noel E, Fantino O, Perrin-Fayolle O, Tran-Minh VA (1999) Magnetic resonance imaging findings in idiopathic adhesive capsulitis of the shoulder. Rev Rhum Engl Ed 66: 201-206.
- Connell D, Padmanabhan R, Buchbinder R (2002) Adhesive capsulitis: role of MR imaging in differential diagnosis. Eur Radiol 12: 2100-2106.
- Mengiardi B, Pfirrmann CW, Gerber C, Hodler J, Zanetti M (2004) Frozen shoulder: MR arthrographic findings. Radiology 233: 486-492.
- Sofka CM, Ciavarra GA, Hannafin JA, Cordasco FA, Potter HG (2008) Magnetic resonance imaging of adhesive capsulitis: correlation with clinical staging. HSS J 4: 164-169.
- Tamai K, Yamato M (1997) Abnormal synovium in the frozen shoulder: a preliminary report with dynamic magnetic resonance imaging. J Shoulder Elbow Surg 6: 534-543.
- Wiley AM (1991) Arthroscopic appearance of frozen shoulder. Arthroscopy 7: 138-143.
- Yoo JC, Ahn JH, Lee YS, Koh KH (2009) Magnetic resonance arthrographic findings of presumed stage-2 adhesive capsulitis: focus on combined rotator cuff pathology. Orthopedics 32: 22.
- Emig EW, Schweitzer ME, Karasick D, Lubowitz J (1995) Adhesive capsulitis of the shoulder: MR diagnosis. AJR Am J Roentgenol 164: 1457-1459.
- Teefey SA, Rubin DA, Middleton WD, Hildebolt CF, Leibold RA, et al. (2004) Detection and quantification of rotator cuff tears. Comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic findings in seventy-one consecutive cases. J Bone Joint Surg Am 86-A: 708-716.
- Karjalainen PT, Soila K, Aronen HJ, Pihlajamäki HK, Tynninen O, et al. (2000) MR imaging of overuse injuries of the Achilles tendon. AJR Am J Roentgenol 175: 251-260.
- Riley GP, Goddard MJ, Hazleman BL (2001) Histopathological assessment and pathological significance of matrix degeneration in supraspinatus tendons. Rheumatology (Oxford) 40: 229-230.
- Xu Y, Murrell GA (2008) The basic science of tendinopathy. Clin Orthop Relat Res 466: 1528-1538.
- Shaffer B, Tibone JE, Kerlan RK (1992) Frozen shoulder. A long-term follow-up. J Bone Joint Surg Am 74: 738-746.
- Gotoh M, Hamada K, Yamakawa H, Inoue A, Fukuda H (1998) Increased substance P in subacromial bursa and shoulder pain in rotator cuff diseases. J Orthop Res 16: 618-621.