
Journal of Clinical and Investigative Dermatology
Download PDF
Case Report
*Address for Correspondence: Mohammad Ali Alshami, Dermatology Department, Faculty of medicine, and health sciences, Sana’a University, Sana’a, Yemen, Tel: 00967733760082; E-mail: mohammadalshami62@gmail.com
Citation: Alshami MA. A Case of Juvenile Colloid Milium with Atypical Cutaneous Horn like Lesions in a Young Yemeni Patient. J Clin Investigat Dermatol. 2016;4(2): 2.
Copyright © 2016 Alshami MA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Investigative Dermatology | ISSN: 2373-1044 | Volume: 4, Issue: 2
Submission: 08 June, 2016| Accepted: 06 July, 2016 | Published: 11 July, 2016

 Histopathological examination of skin from the cutaneous horn like papule showed pale pink homogenous material in the papillary dermis with typical splitting and fissures and the absence of a Grenz zone. The overlying epidermis was atrophic (Figures 3a and 3b).
Histopathological examination of skin from the cutaneous horn like papule showed pale pink homogenous material in the papillary dermis with typical splitting and fissures and the absence of a Grenz zone. The overlying epidermis was atrophic (Figures 3a and 3b).

A Case of Juvenile Colloid Milium with Atypical Cutaneous Horn like Lesions in a Young Yemeni Patient
Mohammad Ali Alshami*
- Dermatology Department, Faculty of medicine, and health sciences, Sana’a University, Sana’a, Yemen
*Address for Correspondence: Mohammad Ali Alshami, Dermatology Department, Faculty of medicine, and health sciences, Sana’a University, Sana’a, Yemen, Tel: 00967733760082; E-mail: mohammadalshami62@gmail.com
Citation: Alshami MA. A Case of Juvenile Colloid Milium with Atypical Cutaneous Horn like Lesions in a Young Yemeni Patient. J Clin Investigat Dermatol. 2016;4(2): 2.
Copyright © 2016 Alshami MA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Investigative Dermatology | ISSN: 2373-1044 | Volume: 4, Issue: 2
Submission: 08 June, 2016| Accepted: 06 July, 2016 | Published: 11 July, 2016
Abstract
Juvenile colloid milium is a rare degenerative dermatosis of keratinocytes manifesting before puberty. It has a chronic course, is detected primarily over sun-exposed areas, and is clinically characterized by the development of translucent, waxy, yellowishamber papules and plaques containing gelatinous material and(histologically characterized) by the presence of eosinophilic, fissured material in the papillary dermis. We present the case of a 16-yearold Yemeni boy with juvenile colloid milium, who presented with an unusual variant of juvenile colloid milium with waxy transparent papules on the helices which resembled a cutaneous horn. This is the third case report from Yemen as the author has (previously) reported 2 cases in Yemeni sibling(s).Introduction
Colloid milium (CM) is a very rare degenerative dermatosis of the dermal connective tissue and/or keratinocytes. Since its first description by Wagner in 1866, around 150 cases have been reportedworldwide [1,2]. It is clinically characterized by the development of translucent, yellowish-amber papules and plaques, primarily over sun-exposed areas, from which viscous material can be expressed and (histologically characterized) by the presence of eosinophilic fissured material in the papillary dermis [2].There are four recognized variants (adult, juvenile, nodular colloid degeneration, and pigmented types) [2-5]. The juvenile type is typically inherited and manifests before puberty. This type is exceptionally rare, with only 22 cases reported worldwide to date [6]. We present the case of a 16-year-old Yemeni boy with juvenile colloid milium with waxy transparent papules on the helices which resembled a cutaneous horn.
Case Report
A 16-year-old Yemeni boy, presented with skin lesions since the age of 8. He was otherwise healthy, and no other family member has similar skin condition. This patient lived in a rural area and wasfrequently exposed to the sun and petrochemicals (herbicides). He presented with lesions of varying morphologies including waxy (Figures 1a-1d), amber (Figures 2a and 2b), and acrochordon like papules (Figure 2c), and whitish flat papules (Figure 2b). Few flat whitish papules were also present over the dorsum of the index finger (Figure 2d). These lesions had grown gradually with age, both in size and number. The patient also presented with waxy transparent papules over both helices which resembled a cutaneous horn. This feature has not been previously reported in the literature.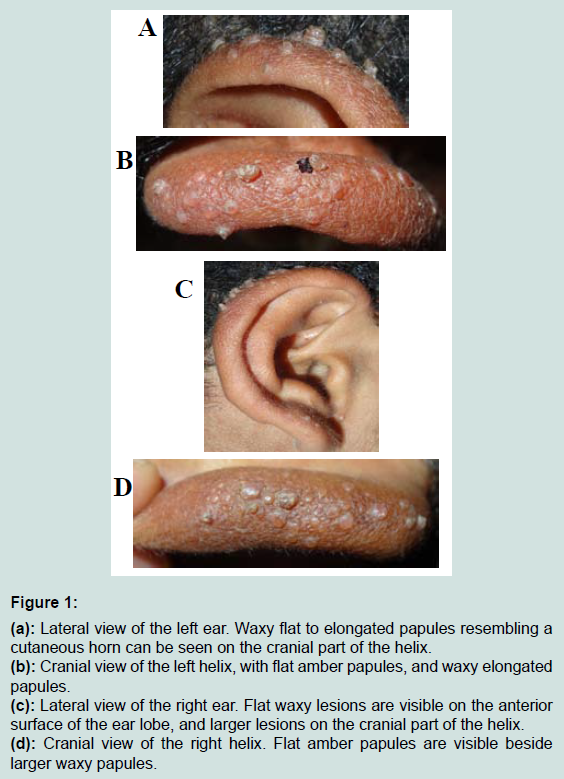
Figure 1: (a): Lateral view of the left ear. Waxy flat to elongated papules resembling a cutaneous horn can be seen on the cranial part of the helix.(b): Cranial view of the left helix, with flat amber papules, and waxy elongated papules.(c): Lateral view of the right ear. Flat waxy lesions are visible on the anterior surface of the ear lobe, and larger lesions on the cranial part of the helix.(d): Cranial view of the right helix. Flat amber papules are visible beside larger waxy papules.
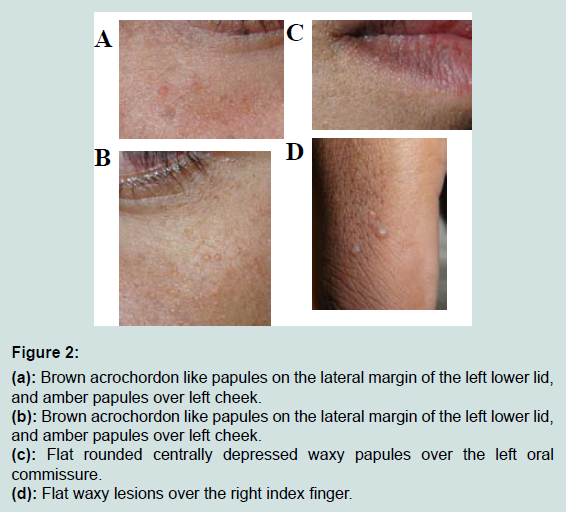
Figure 2: (a): Brown acrochordon like papules on the lateral margin of the left lower lid, and amber papules over left cheek.(b): Brown acrochordon like papules on the lateral margin of the left lower lid, and amber papules over left cheek.(c): Flat rounded centrally depressed waxy papules over the left oral commissure.(d): Flat waxy lesions over the right index finger.
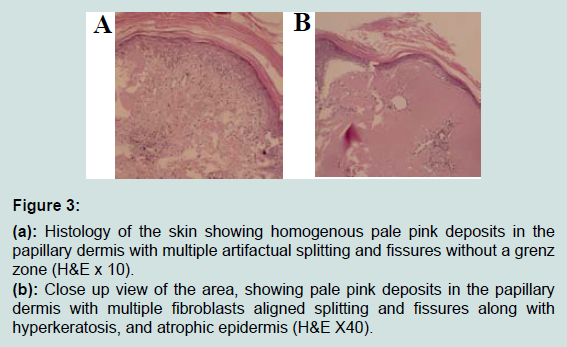
Figure 3: (a): Histology of the skin showing homogenous pale pink deposits in the papillary dermis with multiple artifactual splitting and fissures without a grenz zone (H&E x 10).(b): Close up view of the area, showing pale pink deposits in the papillary dermis with multiple fibroblasts aligned splitting and fissures along with hyperkeratosis, and atrophic epidermis (H&E X40).
Discussion
The adult type of CM develops after excessive sun exposure in adolescents or adults, and the colloid material is thought to generate from damaged elastic fibers. This type is reported most commonly in fair-skinned individuals, albeit it has been reported in darker-skinned individuals and on non-sun-exposed skin [7,8]. It can occur eitherbilaterally or unilaterally, and has been reported in association with beta thalassemia and with vitiligo [9-11]. The juvenile type typically manifests before puberty and is inherited in both an autosomalrecessive and an autosomal-dominant manner. The colloid deposition is thought to originate from abnormal keratinocytes. Nodular colloid type presents with large multiple soft-to-rubbery nodules or plaques forming over sun-exposed areas. Few cases of pigmented CM have been reported to be triggered by a combination of chronic sun exposure and chemical exposure, such as fertilizers or strong bleaching creams [3]. Thus, chronic sun exposure was recognized as a common prompting factor for CM. The role of UVA radiation in the development of colloid milium was supported by a report of the development of CM in a psoriatic patient treated with PUVA [12]. Some authors have proposed a papuloverrucous type as an occupational dermatosis triggered by both sun exposure and long-lasting contact with lubricating oils [4]. The standard treatments for CM include chemical peeling, dermabrasion, cryotherapy, and, newly, ablative and fractional-ablative lasers [13-15].We treated our patient with a combination of a chemical peel for flat lesions and electrocautery for the larger lesions with excellent cosmetic results. He was advised to use sunscreen and to avoid contact with herbicides.
References
- Das WE (1866) Colloid-Milium der Haut. Arch Heilkunde 7: 463-464.
- Pourrabbani S, Marra DE, Iwasaki J, Fincher EF, Ronald LM (2007) Colloid milium: a review and update. J Drugs Dermatol 6: 293-296.
- Gönül M, Cakmak SK, Kiliç A, Gül U, Heper AO (2006) Pigmented coalescing papules on the dorsa of the hands: pigmented colloid milium associated with exogenous ochronosis. J Dermatol 33: 287-290.
- Muscardin LM, Bellocci M, Balus L (2000) Papuloverrucous colloid milium: an occupational variant. Br J Dermatol 143: 884-887.
- Wooldridge WE, Frerichs JB (1960) Amyloidosis: a new clinical type. Arch Dermatol 82: 230-234.
- Chowdhury MM, Blackford S, Williams S (2000) Juvenile colloid milium associated with ligneous conjunctivitis: report of a case and review of the literature. Clin Exp Dermatol 25: 138-140.
- Martorell-Calatayud A, Balmer N, Sanmartin O, Botella-Estrada R, Requena C, et al. (2011) Familial juvenile colloid milium: report of a well-documented case. J Am Acad Dermatol 64: 203-206.
- Lim C, Li M (2006) Colloid milium arising on a non-sun-exposed area in an adult. Australas J Dermatol 47: 137-138.
- Giordano G, Ricci R, Froio E, Izzi G, Barone A, et al. (2008) A case of colloid milium in patient with beta thalassaemia major. J Cutan Pathol 35: 566-569.
- Kalantaevskaia KA (1951) Case of colloid milium associated with vitiligo. Vestn Venerol Dermatol 6: 36-38.
- Lewis AT, Le EH, Quan LT, Krishnan B, Schulmeier J, et al. (2002) Unilateral colloid milium of the arm. J Am Acad Dermatol 46 (2 Suppl Case Reports): S5-S7.
- Hashimoto K, Kumakiri M (1979) Colloid-amyloid bodies in PUVA-treated human psoriatic patients. J Invest Dermatol 72: 70-80.
- Netscher DT, Sharma S, Kinner BM, Lyos A, Griego RD (1996) Adult-type colloid milium of hands and face successfully treated with dermabrasion. South Med J 89: 1004-1007.
- Ammirati CT, Giancola JM, Hruza GJ (2002) Adult-onset facial colloid milium successfully treated with the long-pulsed Er:YAG laser. Dermatol Surg 28: 215-219.
- Marra DE, Pourrabbani S, Fincher EF, Moy RL (2007) Fractional photothermolysis for the treatment of adult colloid milium. Arch Dermatol 143: 572-574.