
Journal of Forensic Investigation
Download PDF
Research Article
*Address for Correspondence: Rashmi Metgud, Professor and HOD, Oral & Maxillofacial Pathology and Microbiology, Pacific Dental College & Hospital, Debari, Udaipur-313024, India, Tel: +91-9001829425; E-mail: rashmi_metgud@rediffmail.com
Citation: Metgud R, Bari S, Vyas Z, Tak A. Rugae Profiling: A Pilot Study in Udaipur, Rajasthan. J Forensic Investigation. 2016; 4(1): 4.
Copyright © 2016 Rashmi M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Forensic Investigation | ISSN: 2330-0396 | Volume: 4, Issue: 1
Submission: 24 November, 2015 | Accepted: 18 February, 2016 | Published: 22 February, 2016

 • There was a statistically significant difference in the circular and convergence pattern of rugae which was found to be higher among females than males (p<0.05) (Table 2).
• There was a statistically significant difference in the circular and convergence pattern of rugae which was found to be higher among females than males (p<0.05) (Table 2).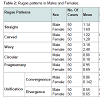 • The Wavy pattern was found to be higher in Udaipur (Table 2).
• The Wavy pattern was found to be higher in Udaipur (Table 2).
Rugae Profiling: A Pilot Study in Udaipur, Rajasthan
Rashmi Metgud*, Samiha Bari, Zankhana Vyas and Anirrudh Tak
- Oral & Maxillofacial Pathology and Microbiology, Pacific Dental College & Hospital, Udaipur, India
*Address for Correspondence: Rashmi Metgud, Professor and HOD, Oral & Maxillofacial Pathology and Microbiology, Pacific Dental College & Hospital, Debari, Udaipur-313024, India, Tel: +91-9001829425; E-mail: rashmi_metgud@rediffmail.com
Citation: Metgud R, Bari S, Vyas Z, Tak A. Rugae Profiling: A Pilot Study in Udaipur, Rajasthan. J Forensic Investigation. 2016; 4(1): 4.
Copyright © 2016 Rashmi M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Forensic Investigation | ISSN: 2330-0396 | Volume: 4, Issue: 1
Submission: 24 November, 2015 | Accepted: 18 February, 2016 | Published: 22 February, 2016
Abstract
Background:Human identification either living or dead is a complex process and one of the main objective of forensic science. The most reliable method of identification is finger printing and DNA profiling, since no two sets of prints are alike. Finger print is most reliable tool provided it is obtained prior to decomposition of body and is not mutilated. It is of little value when body is identified 48 hrs after death or when it has burns, crush injury or had been under water for long. Therefore in such incidences where the routinely used methods of identification are compromised palatal rugae pattern can be used for personal identification.Aim and objective:To study the rugae pattern in a sample of male and female population of Udaipur and to compare the patterns between the two groups, which may be an additional method of determining gender by using maxillary casts.
Materials and methods: The rugae pattern of 50 males and 50 females belonging to Udaipur was studied on maxillary casts.
Results: The Wavy pattern was found to be higher in Udaipur. There was no statistically significant difference in the mean value of number of rugae in males and females. There was a statistically significant difference in the circular and convergence pattern of rugae which was found to be higher among females than males (p<0.05).
Conclusion: The rugae patterns are genetically determined. The findings suggest that rugae are specific to a particular population and might have better utility in population differentiation. This method is simple and inexpensive to conduct and therefore can be applied in forensic odontology.
Keywords
Rugae pattern; Udaipur population differentiationIntroduction
Identification of humans is a prime requisite for certification of death and for personal, social, legal and humanitarian reasons. Many events that take place in the human journey between the womb to the tomb result in human destruction. Violent and heinous activities shatter the lives of the victims, their relatives and families every day. Through the speciality of forensic odontology dentists play a little yet very important role in identification of victims of crime and disaster through dental records. Dental records may be inconclusive, as they may be incomplete as additional treatment might have been performed in time interval of creation of dental record and death of patient.Rugoscopy, the study of palatal rugae can be used for individual identification and necro identification. Rugae are asymmetrical and irregular elevations of the mucosa located on the anterior third of palate. Studies have demonstrated that no two palates are alike in their configuration and that the characteristic pattern of the palate does not change as a result of growth [1]. They are protected from trauma by their internal position in the head and insulated from heat by tongue and buccal pads of fat [2]. Analysis of variables which make up the classification of rugae pattern contributes to individuality of rugae in different populations [3]. In genetically similar populations, rugae measurements may be inconclusive and hence rugae patterns can be helpful. Rugoscopy is advantageous over other methods because of its low cost, ease of use and can be used in cases of burns and decomposition where other methods of identification are compromised [4].
Aim and objective
1) To study the rugae pattern in a sample of male and female population of Udaipur, Rajasthan.2) To compare the patterns between the two groups, which may be an additional method of determining gender.
Material and Methods
The sample comprised of 100 maxillary casts of 50 males and 50 females of an age group ranging from 12-30 years belonging to Udaipur, Rajasthan. They were randomly selected from Department Of Orthodontics, Pacific Dental College and Hospital, Udaipur, India. Exclusion criteria was children below the age of 12 years, presence of thumb sucking habit, existence of palatal lesion, congenital palatal deformity, orthodontic treatment and history of palatal surgery. The rugae were highlighted using a graphite pencil and the no. of rugae were counted and patterns were recorded according to classification given by Thomas and Kotze (Figure 1) [5].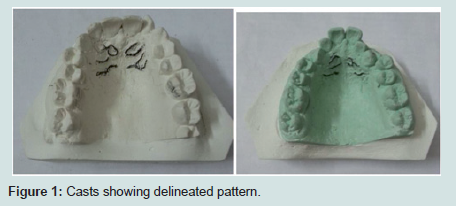
Figure 1: Casts showing delineated pattern.
Statistical analysis
• Two-sample t‑test and Chi-Square tests were used for comparison of means in male and female subjects.• A significance level of 5% was considered as critical value.
Results
• There was no statistically significant difference in the mean value of number of rugae in males and females (Table 1).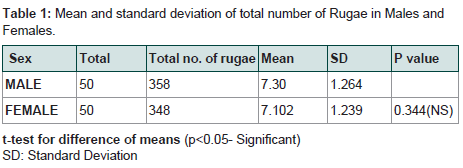
Table 1: Mean and standard deviation of total number of Rugae in Males and Females.
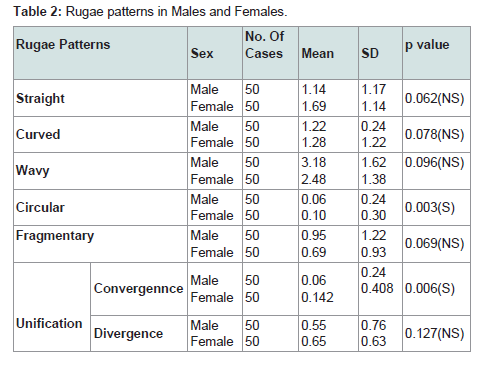
Table 2: Rugae patterns in Males and Females.
Discussion
Transverse palatine folds or palatal rugae (PR) are asymmetrical and irregular elevations of the mucosa in the anterior third of the palate, arranged in a transverse direction from the palatine raphe located in the mid-sagittal plane [6,7]. Palatal rugae appear during the third month of intrauterine life from the connective tissue covering the palatine process of the maxillary bone [8]. English et al., [9] and Peavy and Kendrick [10] noted that the characteristic pattern of the palatal rugae did not change as a result of growth, remaining stable from the time of development until the oral mucosa degenerated at death. Van der Linden proved that the anterior rugae do not increase in length after 10 years of age. The qualitative characteristics like shape, unification and pattern remains same throughout life [11].Thomas and Kotze studied the rugae patterns of 6 South African populations to analyze the interracial difference. Their results indicate that rugae were unique to each ethnic group and can be used successfully as a medium for genetic research [5]. India is a country of genetic complexity. It does not always correlate to ethnicity, geography, or language. Therefore for creating forensic database in India instead of broad grouping of populations; differentiating small, well defined, clusters of populations is more helpful. The present study was taken up in view of the limited existing studies on rugae patterns in Indian populations, with an aim to study and compare the shape of palatal rugae in Udaipur population.
Studies have shown that trauma, thumb sucking habit in infancy, persistent pressure from orthodontic treatment and dentures may lead to changes in the rugae pattern [12]. Thus these factors were considered in exclusion criteria.
In the present study, the wavy pattern followed by straight was found to be higher in Udaipur population.
The results were consistent with the studies conducted in various part of India by Rachna Rath and Ajay Reginald [12], Eshani Saxena et al., [13]. Swetha S [14], Shetty DK et al., [15], Reddy et al., [16], S. Bhagwath, L. Chandra [17], Rezwana Begum Mohammed et al., [18], Suersh Babu et al., [19], Shubha C et al., [20], Kumar S et al., [21], S. Manjunath et al., [22], Mahabalesh Shetty [23], A. Saraf et al., [24] where wavy pattern was found to be most prevalent. The results were in contrast with the studies conducted by Baligi P et al., [25] and Kamala R et al. [26], where straight and curve pattern were found to be most prevalent respectively (Table 3). The sinuous and curve rugae pattern were observed in Caucasian and Aboriginal Australians (Kapali et al.,) [227]. The unification pattern was found to be more in Chinese individuals (Reddy et al., [16]), Shetty et al. [28] found that in Indian males more number of curved rugae on both right and left sides was observed than Tibetan males. Also Tibetan females had more wavy rugae on right and left sides than Indian females. Studies by Nayak et al. [29] suggested that Southern Indians showed more number of straight and curved rugae than Western Indians. Similarly Paliwal et al., [30], found that Kerala population showed predominant straight rugae pattern on the right side of the palate among males when compared to Madhya Pradesh population. The aforementioned literature suggests that the rugae patterns are unique to certain populations.
The sinuous and curve rugae pattern were observed in Caucasian and Aboriginal Australians (Kapali et al.,) [227]. The unification pattern was found to be more in Chinese individuals (Reddy et al., [16]), Shetty et al. [28] found that in Indian males more number of curved rugae on both right and left sides was observed than Tibetan males. Also Tibetan females had more wavy rugae on right and left sides than Indian females. Studies by Nayak et al. [29] suggested that Southern Indians showed more number of straight and curved rugae than Western Indians. Similarly Paliwal et al., [30], found that Kerala population showed predominant straight rugae pattern on the right side of the palate among males when compared to Madhya Pradesh population. The aforementioned literature suggests that the rugae patterns are unique to certain populations.
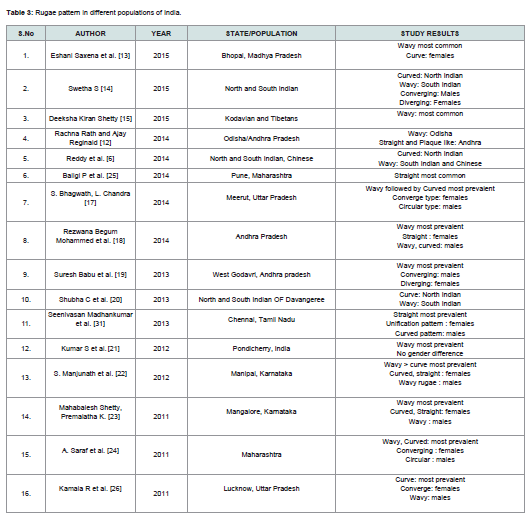
Table 3: Rugae pattern in different populations of India.
In the present study, circular and convergence patterns were found to be higher in females of Udaipur than males. The result was consistent with studies conducted by A. Saraf et al., [24] and S. Bhagwath, L. Chandra [17], where convergence pattern was more prevalent in females than males. Studies done by Rezwana Begum Mohammed et al., [18], Seenivasan Madhankumar et al., [31], S. Manjunath et al., [22], and Mahabalesh Shetty, Premalatha K [23], showed that straight, unification and curved and straight pattern respectively were prevalent in females (Table 3). However in the present study the sample size was small so nothing much can be commented on the gender differentiation potential of rugae pattern.
The wavy pattern was found to be the most common in Udaipur. However the females in Udaipur had more circular and convergence pattern as compared to males. Though this difference came out to be statistically significant but as the sample size taken was too small so commenting on the gender differentiation potential of rugae pattern isn’t helpful. Therefore study on a larger sample size is needed to prove this gender difference. However this difference can be helpful in differentiating the people of Udaipur from other Indian populations where wavy pattern was found to be most common.
Thus the present study supported previous reports that palatal rugae played a significant role in population differentiation and could be used as genetic marker for research on population groups.
Conclusion
The rugae patterns are genetically determined. The findings suggest that rugae are specific to a particular population and might have better utility in population differentiation. In the present study following observations were drawn:1) Wavy pattern was found to be more prevalent in Udaipur.
2) Convergence and circular pattern was found more in females than males.
This method is simple and inexpensive to conduct and therefore can be applied in forensic odontology.
References
- Limson KS, Julian R (2004) Computerized recording of the palatal rugae pattern and an evaluation of its application in forensic identification. J Forensic Odontostomatol 2004: 22: 1-4.
- Lebret L (1962) Growth changes of the palate. J Dent Res 41: 1391-1404.
- Ohtani M, Nishida N, Chiba T, Fukuda M, Miyamoto Y, et al. (2008) Indication and limitations of using palatal rugae for personal identification in edentulous cases. Forensic Sci Int 176: 178-182.
- Nayak P, Acharya AB, Padmini AT, Kaveri H (2007) Differences in the palatal rugae shape in two populations of India. Arch Oral Biol 52: 977-982.
- Thomas CJ, Kotze TJ (1983) The palatal ruga pattern: a new classification. J Dent Assoc S Afr 38: 153-157.
- Patil MS, Patil SB, Acharya AB (2008) Palatine rugae and their significance in clinical dentistry: a review of the literature. J Am Dent Assoc 139: 1471-1478.
- Caldas IM, Magalhaes T, Afonso A (2007) Establishing identity using cheiloscopy and palatoscopy. Forensic Sci Int 165: 1-9.
- Amasaki H, Ogawa M, Nagasao J, Mutoh K, Ichihara N, et al. (2003) Distributional changes of BrdU, PCNA, E2F1 and PAL31 molecules in developing murine palatal rugae. Ann Anat 185: 517-523.
- English WR, Robison SF, Summitt JB, Oesterle LJ, Brannon RB, et al. (1988) Individuality of human palatal rugae. J Forensic Sci 33: 718-726.
- Peavy DC Jr, Kendrick GS (1967) The effects of tooth movement on the palatine rugae. J Prosthet Dent 18: 536-542.
- van der Linden FP (1978) Changes in the position of posterior teeth in relation to ruga points. Am J Orthod 74: 142-161.
- Rath R, Reginald BA (2014) Palatal rugae: An effective marker in population differentiation. J Forensic Dent Sci 6: 46-50.
- Saxena E, Chandrashekhar BR, Hongal S, Torwane N, Goel P, et al. (2015) A study of the palatal rugae pattern among male female and transgender population of Bhopal city. J Forensic Dent Sci 7: 142-147.
- Swetha S (2015) Palatal rugae pattern in varied adult Indian population of males and females. J Pharm Sci Res 7: 736-739.
- Shetty DK, Mali S, Divakar HD, Amit P, Dhairaysheel E, et al. (2015) Palatal rugae patterns as a bioindicator for forensic identification in Kodava and Tibetan populations of India. J Int Oral Health 7 (Suppl 2): 57-59.
- Reddy SV, Gautam NS, Rao TH , Gautam NR, Koganti R, et al. (2014) Comparison of palatal rugae pattern among North Indian, South Indian and Chinese students of Manipal university 4: 40-44.
- Bhagwath S, Chandra L (2014) Rugae pattern in a sample of population of Meerut - An institutional study: J Forensic Dent Sci 6: 122-125.
- Mohammed RB, Rao TH, Rani GS, Chowdary MS, Prasanthi B, et al. (2014) Analysis of various rugae patterns among Coastal Andhra (South Indian) population: digitized method. Oral Maxillofac Pathol J 5: p418.
- Babu GS, Bharath TS, Kumar NG (2013) Characteristics of Palatal Rugae Patterns in west godavari population of India. J Clin and Diagn Res 7: 2356-2359.
- Shubha C, Sujatha GP, Ashok L, Santhosh CS (2013) A study of palatal rugae pattern among North and South Indian population of Davanagere city. J Indian Acad Forensic Med 35: 3.
- Kumar S, Vezhavendhan N, Shanthi V, Balaji N, Sumathi MK, et al. (2012) Palatal rugoscopy among Puducherry population. J Contemp Dent Pract 13: 401-404.
- Manjunath S, Bakkannavar SM, Pradeep Kumar G, Bhatt VJ, Prabhu N, et al. (2012) Palatal rugae patterns among the Indians at Manipal, India. J Pharm Biomed Sci 20: 1-5.
- Shetty M, Premalatha K (2011) Study of palatal rugae pattern among the student population in Mangalore. J Indian Acad Forensic Med 33: 2.
- Saraf A, Bedia S, Indurkar A, Degwekar S, Bhowate R (2011) Rugae patterns as an adjunct to sex differentiation in forensic identification; J Forensic Odontostomatol 29: 14-19.
- Balgi P, Bhalekar B, Bhalerao K, Bhide E, Palaskar S, et al. (2014) Study of palatal rugae pattern in gender identification. J Dent Allied Sci 3: 13-16.
- Kamala R, Gupta N, Bansal A, Sinha A (2011) Palatal rugae pattern as an aid for personal identification: a forensic study. J Indian Acad Oral Med Radiol 23: 173.
- Kapali S, Townsend G, Richards L, Parish T (1997) Palatal rugae patterns in Australian aborigines and Caucasians. Aust Dent J 42: 129-133.
- Shetty SK, Kalia S, Patil K, Mahima VG (2005) Palatal rugae pattern in Mysorean and Tibetan populations. Indian J Dent Res 16: 51-55.
- Nayak P, Acharya AB, Padmini AT, Kaveri H (2007) Differences in the palatal rugae shape in two populations of India. Arch Oral Biol 52: 977-982.
- Paliwal A, Wanjari S, Parwani R (2010) Palatal rugoscopy: Establishing identity. J Forensic Dent Sci 2: 27-31.
- Madhankumar S, Natarajan S, Maheswari U, Kumar VA, Padmanabhan TV, et al. (2013) Palatal rugae pattern for gender identification among selected student population in Chennai, India. J Sci Res Reports 2: 491-496.