
Journal of Geriatrics and Palliative Care
Download PDF
are worded in a positive direction, so they were
Research Article
*Address for Correspondence: XinQi Dong, Rush Institute for Healthy Aging, Rush University Medical Center, Chicago, Illinois, USA, Tel: 312 942 3350; Fax: 312 942 2861; E-mail: xinqi_dong@rush.edu
Citation: Dong X, Zhang M. The Association between Filial Piety and Perceived Stress among Chinese Older Adults in Greater Chicago Area. J Geriatrics Palliative Care 2016;4(1): 11.
Copyright © 2016 Dong X, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Geriatrics and Palliative Care | ISSN: 2373-1133 | Volume: 4, Issue: 1
Submission: 03 February 2016 | Accepted: 13 March, 2016 | Published: 22 March 2016
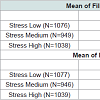
 Table 2 presents means of filial piety expectation and receipt by stress tertiles. The receipt of filial piety was differed by perceived stress tertiles (p< 0.001). The expectation of filial piety was not significantly differed across three perceived stress groups. The receipt of filial was 23.25 (SD=4.52) among the low stress group, compared to 20.90 (SD= 5.32) among the high stress group. The expectation of filial piety was 20.58 (SD=6.06) among the low stress group, compared to 21.09 (SD= 6.01) among the high stress group.
Table 2 presents means of filial piety expectation and receipt by stress tertiles. The receipt of filial piety was differed by perceived stress tertiles (p< 0.001). The expectation of filial piety was not significantly differed across three perceived stress groups. The receipt of filial was 23.25 (SD=4.52) among the low stress group, compared to 20.90 (SD= 5.32) among the high stress group. The expectation of filial piety was 20.58 (SD=6.06) among the low stress group, compared to 21.09 (SD= 6.01) among the high stress group.
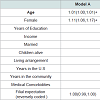
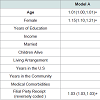
 The associations between expectations of filial piety and perceived stress are presented in Table 3. Expectation of filial piety is not associated with higher levels of perceived stress after adjusting for age, sex, education, income, marital status, number of children, living arrangement, years in the U.S, years in the community, and medical comorbidities. In contrast, perceived receipt of filial piety was associated with higher levels of perceived stress. In the fully adjusted model (Model E), every 1 point lower in receipt of filial piety (range 6-30) score was associated with 3% higher in perceived stress (rang 0-40, Rate Ratio: 1.03, 1.03-1.04) after all the confounding variables were controlled.
The associations between expectations of filial piety and perceived stress are presented in Table 3. Expectation of filial piety is not associated with higher levels of perceived stress after adjusting for age, sex, education, income, marital status, number of children, living arrangement, years in the U.S, years in the community, and medical comorbidities. In contrast, perceived receipt of filial piety was associated with higher levels of perceived stress. In the fully adjusted model (Model E), every 1 point lower in receipt of filial piety (range 6-30) score was associated with 3% higher in perceived stress (rang 0-40, Rate Ratio: 1.03, 1.03-1.04) after all the confounding variables were controlled.
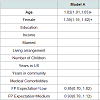
 In the logistic regression models Tables 4a and 4b, higher levels of filial piety expectation was not associated with higher odds of perceiving stress as high. However, higher level of filial piety receipt was associated with higher odds of perceiving stress as high. In the final model where potential confounding factors were controlled, older adults who received a medium level of filial piety were 1.57 (1.29-1.93) times more likely to perceive stress as high, compared with older adults who received a high level of filial piety receipt. Olderadults received a low level of filial piety were 2.74 (2.26-3.33) times more likely to perceive stress as high, compared with older adults who received a high level of filial piety receipt.
In the logistic regression models Tables 4a and 4b, higher levels of filial piety expectation was not associated with higher odds of perceiving stress as high. However, higher level of filial piety receipt was associated with higher odds of perceiving stress as high. In the final model where potential confounding factors were controlled, older adults who received a medium level of filial piety were 1.57 (1.29-1.93) times more likely to perceive stress as high, compared with older adults who received a high level of filial piety receipt. Olderadults received a low level of filial piety were 2.74 (2.26-3.33) times more likely to perceive stress as high, compared with older adults who received a high level of filial piety receipt.
 In the logistic regression models Tables 5a and 5b, no associations were found between the expectation of filial piety and perceived stress. Significant associations were found between the receipt of filial piety and perceived stress. Compared to older adults with a low level of perceived stress and a high level of filial piety, older adults received a low level of filial piety and a medium level of filial piety were respectively 3.43 (2.75-4.28) and 1.69 (1.34-2.12) times more likely to perceive stress as high. Similarly, compared with older adults who had a low level of perceived stress and a high level of filial receipt, older adults received a low level of filial piety and a medium level of filial piety were respectively 1.20 (1.10,1.30) and 1.58 (1.27-1.96) times more likely to perceive stress as medium.
In the logistic regression models Tables 5a and 5b, no associations were found between the expectation of filial piety and perceived stress. Significant associations were found between the receipt of filial piety and perceived stress. Compared to older adults with a low level of perceived stress and a high level of filial piety, older adults received a low level of filial piety and a medium level of filial piety were respectively 3.43 (2.75-4.28) and 1.69 (1.34-2.12) times more likely to perceive stress as high. Similarly, compared with older adults who had a low level of perceived stress and a high level of filial receipt, older adults received a low level of filial piety and a medium level of filial piety were respectively 1.20 (1.10,1.30) and 1.58 (1.27-1.96) times more likely to perceive stress as medium.

The Association between Filial Piety and Perceived Stress among Chinese Older Adults in Greater Chicago Area
XinQi Dong* and Manrui Zhang
- Rush Institute for Healthy Aging, Rush University Medical Center, Chicago, Illinois, USA
*Address for Correspondence: XinQi Dong, Rush Institute for Healthy Aging, Rush University Medical Center, Chicago, Illinois, USA, Tel: 312 942 3350; Fax: 312 942 2861; E-mail: xinqi_dong@rush.edu
Citation: Dong X, Zhang M. The Association between Filial Piety and Perceived Stress among Chinese Older Adults in Greater Chicago Area. J Geriatrics Palliative Care 2016;4(1): 11.
Copyright © 2016 Dong X, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Geriatrics and Palliative Care | ISSN: 2373-1133 | Volume: 4, Issue: 1
Submission: 03 February 2016 | Accepted: 13 March, 2016 | Published: 22 March 2016
Abstract
Background: Perceived stress influences the health and well-being of older adults. This study aims to examine the association between the expectation and the receipt of filial piety and perceived stress among U.S Chinese older adults.Methods: Data were drawn from the PINE study, a populationbased study of Chinese older adults aged 60 and above in the greater Chicago area. Perceived stress was assessed by the PSS-10 and was the dependent variable. Independent variables were the expectation and the receipt of filial piety examined in six domains. Negative Binomial Regression and Multivariable Logistic Regression analyses were conducted.
Results: Of the 3,159 Chinese older adults interviewed, the mean age was 72.8 (SD=8.3) and 58.9% were female. Compared with older adults who received a high level of filial piety, older adults who received a medium level of filial piety were 1.57 (1.29-1.93) times more likely to perceive stress as high, and older adults who received a low level of filial piety were 2.74 (2.26-3.33) times more likely to perceive stress as high, after controlling for the potential confounding variables. The expectation of filial piety was not significantly associated with perceived stress.
Conclusion: A low level of filial piety receipt may be a risk factor for perceived stress. Our findings suggest incorporating cultural contributors into the analyses of perceived stress.
Keywords
Population studies; Perceived stress; Filial piety: Chinese agingIntroduction
Perceived stress is an important health indicator. An individual perceives stress when they encounter situations that exceed their capability to deal with [1]. Unmanaged stress has negative influences on physical and mental health [2-5]. Aging process exposes older adults to some new type of stressors, and enervates their capability to cope [6]. For instance, older adults are more likely to live with one or more chronic health conditions, with accelerating healthcare expenditures and limited income [7,8]. Negative perceptions towardold age also cause a great number of psychological stressors among older adults, such as the fear of loss, anxiety over aging, concerns on physical appearance, etc. [9,10]. Many older adults are unfamiliar with those emerging stressors and their previous skills and experiences contribute little to stress coping [11]. Previous study indicates that chronic exposure to stress renders more severe health effects on older adults [12].Older immigrants are prone to stress because they are often disadvantaged in terms of social capital, human capital, language proficiency, and cultural adaptability [13-15]. Despite the above mentioned facets, older immigrants are often less likely to succeed in acquiring necessary coping resources in the mainstream culture [16]. Cultural, linguistic, and systematic barriers may impede this population from seeking and obtaining external assistance in U.S society [17,18]. Currently, scads of research efforts emphasized the consequences of stress and the underlying bio-physiological mechanism through which stress influences health of humans [2-4]. Meanwhile, a growing body of literature examined the social and behavioral risk factors of perceived stress, such as age, gender, income, education, health conditions, living arrangement, marital status etc. [19-22]. However, cultural determinants of perceived stress have not been well explored, although it was recognized in prior study that culture values influence health and well-being of older adults [23,24]. Current literature indicates that Chinese traditional values and norms shape the way of thinking, and thus affect mind-body interaction and the state of physical and mental health [25]. Specifically, one study pointed out that culture influences how stressors are defined and perceived, and how coping resources and support are recognized and acquired [26].
With a population of more than four million, the Chinese population has experienced rapid growth in the U.S in recent years [27]. The mean age of Chinese population is relatively older than other populations, with 15% of the total population aged 60 and over. Adjusting lives in the U.S. can be challenging for Chinese older adults since a majority of them are not native-born (80%) and one third of them immigrated to U.S after the age of 60 [28].
Chinese culture has been enforcing filial piety as an important moral standard historically [29]. Filial piety stipulates that adult children within the Chinese families are obligated to take care of older parents, emphasizing reciprocity in the parent-child relationships [30]. Adult children are required to provide adequate support to fulfill the emotional and practical needs of their older parents [30,31]. Filial piety may be associated with perceived stress as it affects both stressors and stress coping. Children who do not perform filial duties are often deemed as the tragedy of the entire family and the misfortune of the older parents [32]. Thus, perceiving children not filial may serve as an intrinsic stressor. Furthermore, considering that filial piety has significant influence on inter-generational relationships and general well-being of older parents [31,33,34], it is likely that filial piety substantially indicates whether older parents can obtain adequate emotional and tangible support from children whenencountering stressful situations.
There can be disagreements between the older parents and adult children in terms of the ideological beliefs and practical delivery of filial care [35], since filial behaviors are usually considered as the reciprocal contracts between two generations. The generational gaps are usually enlarged with the course of immigrating to U.S, a society that values individualism and counts on social welfare system for elder care [14]. The traditional conceptualization of filial piety may have been altered among the younger generations who acculturate at a higher degree. In contrast, their older parents may be more persistent in keeping filial piety belief and practice operating within the family [36]. Hence, there is a risk that some older adults are not able to getdesired filial care, and this group of older adults are vulnerable in faceof stress in late life.
Filial piety still plays important role guiding elder care within the U.S Chinese families [33], considering that more than one third of Chinese older adults reported that they could not cope with things in daily life [37], and primarily rely on children as an important source of social support [38]. Although prior studies have explored extensively regarding the effect of filial piety on intergenerational relationships, the association between filial piety and perceived stress among Chinese older adults is not well documented.
Concerning the negative health consequences associated with stress among older adults, it is important to understand how filial piety contributes to perceived stress among Chinese older adults as it can provide valuable cultural insight for interventions to improve health and well-being among minority populations. Our study aims to examine the association between the expectation and receipt of filial piety and perceived stress. Our central hypothesis is that higher levels of filial piety expectation and filial piety receipt are associated with lower perceived stress after confounding factors are controlled, including socio-demographics, socio-economics, and health measures etc. A better understanding of this issue has important implications in developing culturally appropriate stress coping interventions targeting Chinese older adults in the U.S.
Methods
Population and settingsThe Population Study of Chinese Elderly in Chicago (PINE) is an ongoing population-based epidemiological study of U.S Chinese older adults aged 60 and over in the greater Chicago area. Data in this paper were drawn from the first-wave PINE study data collected in between 2011 to 2013. Briefly, the purpose of the PINE study is to collect community-level data of U.S Chinese older adults to examine key cultural determinants of health and well-being. The project was initiated by a synergistic community-academic collaboration among Rush Institute for Healthy Aging, Northwestern University, and many community-based social services agencies and organizations throughout the greater Chicago area [39].
In order to ensure study relevance to the well-being of the Chinese community and enhance community participation, the PINE study implemented extensive culturally and linguistically appropriate recruitment strategies strictly guided by communitybased participatory research (CBPR) approach [40,41]. Older adults aged 60 and above who self identified as Chinese and reside in Greater Chicago area are eligible to participate in the PINE study. With over twenty social services agencies, community centers, health advocacy agencies, faith-based organizations, senior apartments and social clubs serving as the basis of study recruitment sites, eligible participants were approached through routine social services and outreach efforts targeting Chinese American families in the Chicago city and suburban areas. Out of 3,542 eligible participants, 3,159 agreed to participate in the study, yielding a response rate of 91.9%.
Based on the available census data drawn from U.S Census 2010 and a random block census project conducted in the Chinese community in Chicago, the PINE study is representative of the Chinese aging population in the greater Chicago area with respect to key demographic attributes including age, sex, income, education, number of children, and country of origin [42]. The study was approved by the institutional review board of the Rush University Medical Center.
Measurements
Perceived stressWe used the Perceived Stress Scale (PSS-10) to assess the degree to which situations in lives are perceived as stressful among the Chinese older adults [43,44]. The PSS-10 consists of ten items and each of them assesses how unpredictable, uncontrollable, and overloading respondents felt in their lives. Participants were asked in last month, how often have they felt: (1) upset because of something happened unexpectedly; (2) unable to control important things in life; (3) nervous and stressed; (4) confident about the ability to handle personal problems; (5) things were going your way; (6) could not cope with all the things had to do; (7) been able to control irritations in life; (8) were on top of things; (9) angered because of things happened out of control; 10) could not overcome piled up difficulties. Respondents indicated answers to each question on a 5-point scale ranging from 0=never to 4=very often. Of the 10 items, 4 items (items 4,5,7,8) are worded in a positive direction, so they were reverse scored.
The scores of each item were then summed up and the total score ranged from 0 to 40, with higher scores indicating greater psychological stress. The tertiles of perceived stress among study sample were then calculated and were labeled as “low stress” group, “medium stress” group, and “high stress” group. Content validity was assessed by a group of bilingual and bicultural study researchers and experts in both Chinese cultural issues and health and aging topics. Internal reliability (Cronbach’s alpha) of PSS-10 was estimated to be 0.86 among the Chinese older adults in the U.S [45].
Filial piety: The assessment was planned around six domains of filial piety, including respect, happiness, care, greetings, obedience, and financial support, based on the conceptual model proposed by Gallois and colleagues [46]. On a five-point-scale (1=very little; 2=rather little; 3=average; 4=rather a lot; 5=very much), participants were asked how much care, respect, happiness, obedience, financial support, and how many greetings they expected from their children. Similarly, participants were then asked to evaluate their actual receipt of care, respect, greetings, happiness, obedience, and financial support(1=very little; 5=very much).
The scores of each domain were then summed up and the aggregate score ranged from 6-30, with higher scores indicating greater filial piety expectation or filial piety receipt. The aggregate filial piety scores were reversely coded in the negative binomial regressions where rate ratios were calculated. The tertiles of filial piety expectation among study sample were calculated and were labeled as “low filial piety expectation” group, “medium filial piety expectation” group, and “high filial piety expectation” group. Similarly, the tertiles of filial piety receipt were also calculated and labeled as “low filial piety receipt” group, “medium filial piety receipt” group, and “high filial piety receipt” group. Internal reliability of the scale was 0.88 in our study sample [45].
Confounding factors: Basic socio-demographics and socioeconomics were collected including age, sex, education, annual personal income, marital status, number of children, living arrangement, years in the U.S, years in the community. Education was assessed by asking participants the years of highest educational level completed, ranging from 0 to 17 years or more. Living arrangement was assessed by asking participants how many people live in their household besides themselves and was categorized into three groups: (1) living alone; (2) living with 1-2 persons; (3) living with 2-3 persons; (4) living with 4 more persons. Income groups were divided into four groups: (1) $0-$4,999 per year; (2) $5,000-$9,000 per year; (3) $10,000-14,999 per year; (4) more than $15,000 per year.
Medical comorbidities: Participants were asked if they had been told by a doctor, nurse or therapist that they had: (1) heart disease, heart attack, coronary thrombosis, coronary occlusion or myocardial infarction; (2) stroke or brain hemorrhage; (3) cancer, malignancy or a tumor of any type; (4) high cholesterol; (5) diabetes, sugar in the urine, or high blood sugar; (6) high blood pressure; (7) a broken or fractured hip; (8) thyroid disease; or (9) osteoarthritis or inflammation or problems with joints. The number of medical comorbidities was calculated by totaling the number of “yes” responses to the nine items above.
Data Analysis
Descriptive statistics were used to summarize sociodemographics, socio-economics, and health measures by stress tertiles. Chi-square tests were used to compare whether the means of the filial piety expectation and the means of filial piety receipt differed across stress tertiles. Negative Binomial Regression and Logistic Regression analyses were used to examine the associations between the expectation and receipt of filial piety and perceived stress, controlling for potential confounding factors. Model A was adjusted for age and gender. The next model (model B) was additionally adjusted for education and income. In model C, we added number of children and living arrangement to the previous model. In model D, we added years in the U.S and years in the community to the previous model. In the final model, we furthermore controlled for number of medical comorbidities on the basis of previous models. All of the above models (Models A-E) tested the association between the expectation and receipt of filial piety and perceived stress. Rate ratios (RRs), Odds Ratios (ORs), 95% confidence intervals (CIs), and significance levels were reported. All statistical analyses were conducted using SAS, Version 9.2 (SAS Institute Inc., Cary, NC).Results
Of the 3,159 Chinese older adults interviewed, mean age was 72.8 years (SD=8.3, range 60-105) and 58.9% were female. Table 1 presents socio-demographics, socio-economics, and health measures of our participants by levels of the perceived stress. The levels of perceived stress were differed by age (p< 0.05), gender (p < 0.001), education (p< 0.05), income (p< 0.01), years in the community (p< 0.01), and medial comorbidities (p< 0.001). A high level of stress is more commonly reported among participants who are 75 and older (42.10%), male (63.61%), with 6 years of education or below (45.83%), with annual income 10,000 or below (88.03%), having lived in the community for less than 10 years (60.13%), and with three or more chronic conditions (43.24%).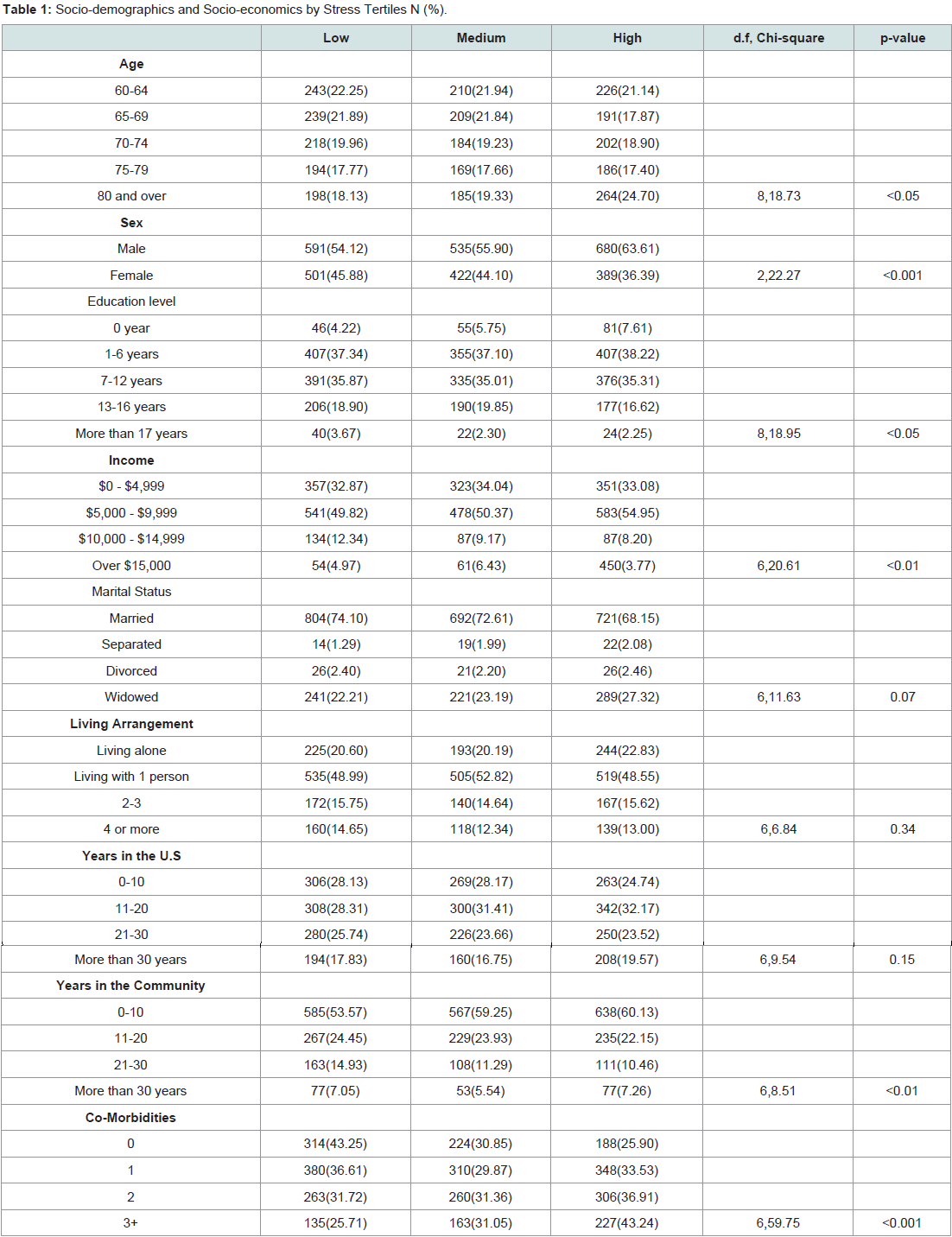
Table 1: Socio-demographics and Socio-economics by Stress Tertiles N (%).
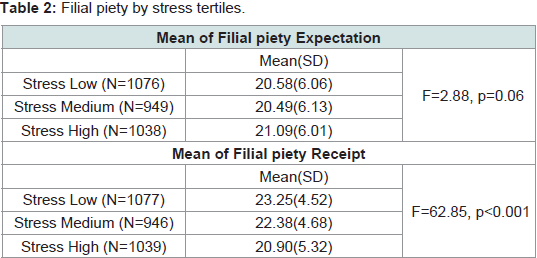
Table 2: Filial piety by stress tertiles.
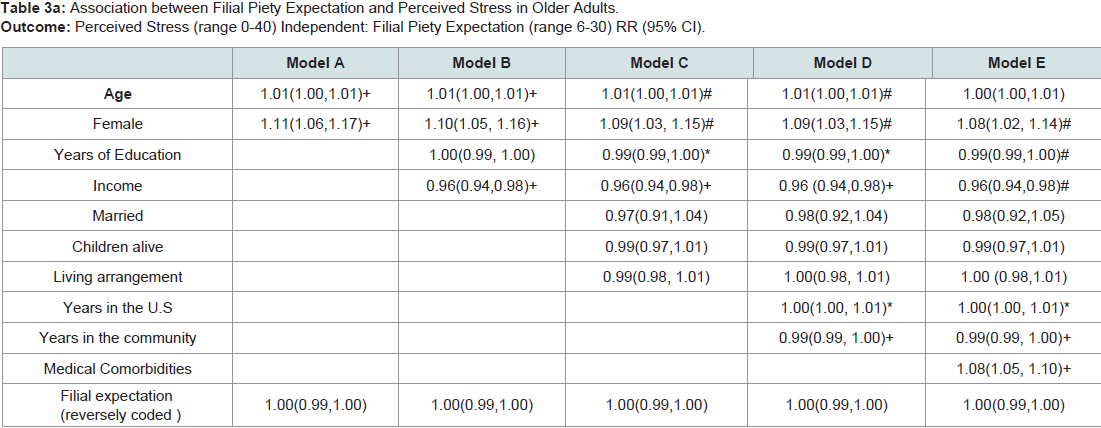
Table 3a: Association between Perceived Stress and Filial Piety Receipt in Older Adults. Outcome: Perceived Stress (range 0-40) Independent: Filial Piety Receipt (range 6-30) RR (95% CI)
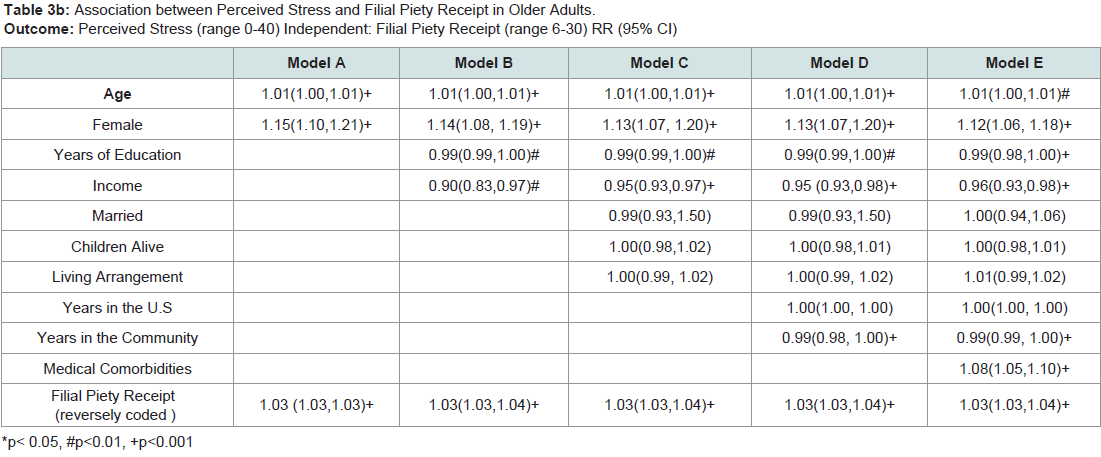
Table 3b: Association between Perceived Stress and Filial Piety Receipt in Older AdultsOutcome: Perceived Stress (range 0-40) Independent: Filial Piety Receipt (range 6-30) RR (95% CI).
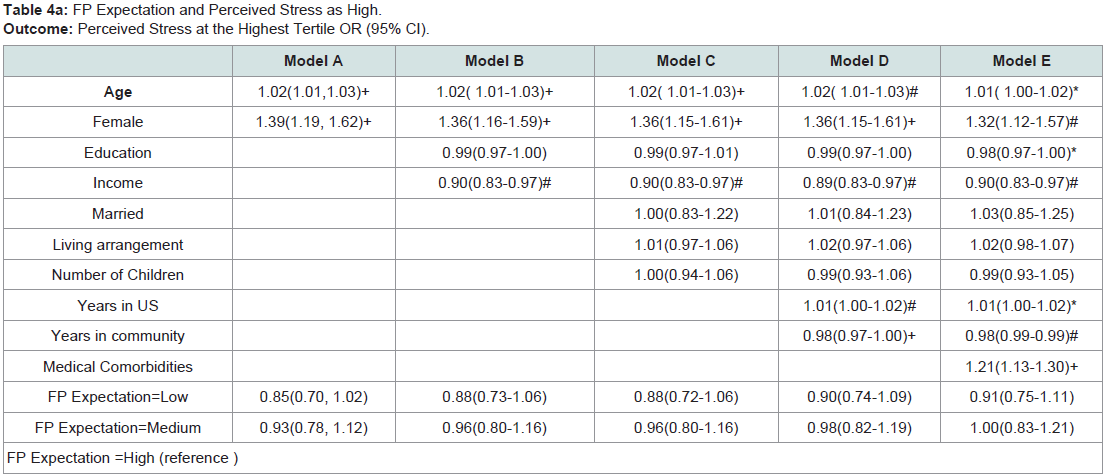
Table 4a: FP Expectation and Perceived Stress as High.Outcome: Perceived Stress at the Highest Tertile OR (95% CI)
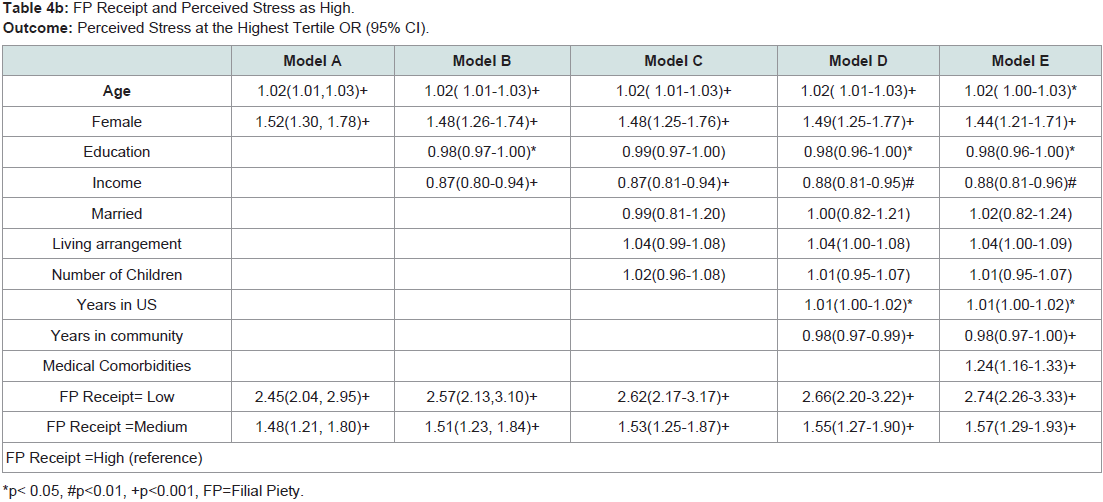
Table 4b: FP Receipt and Perceived Stress as High.Outcome: Perceived Stress at the Highest Tertile OR (95% CI).
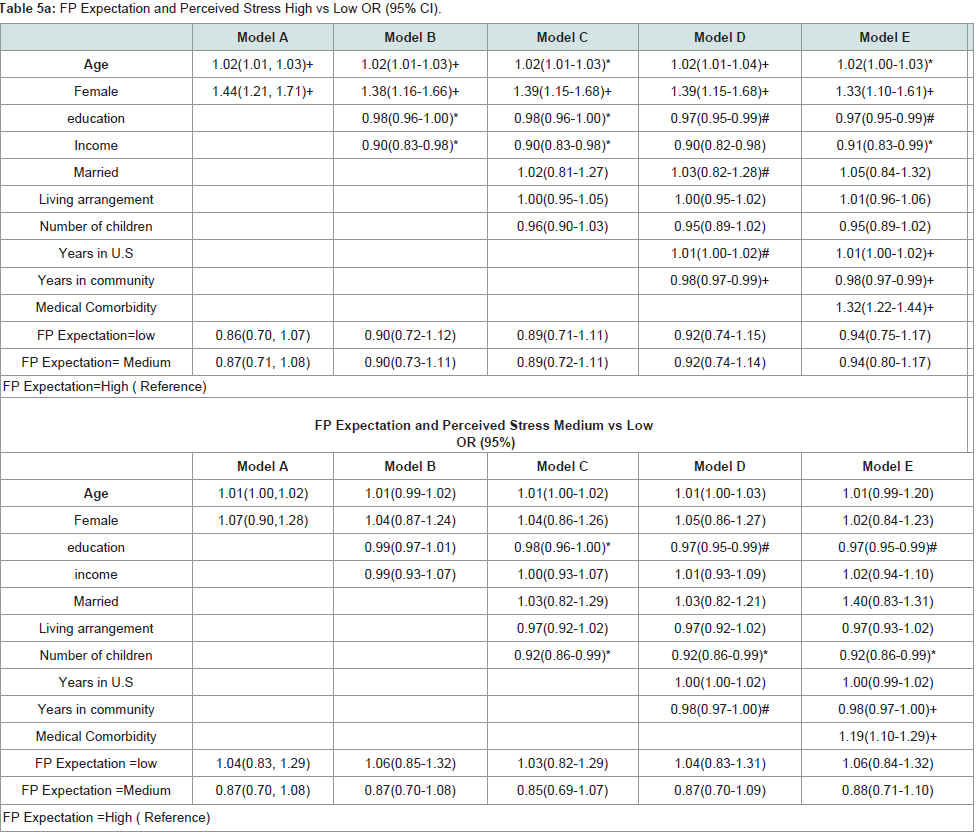
Table 5a: FP Expectation and Perceived Stress High vs Low OR (95% CI).
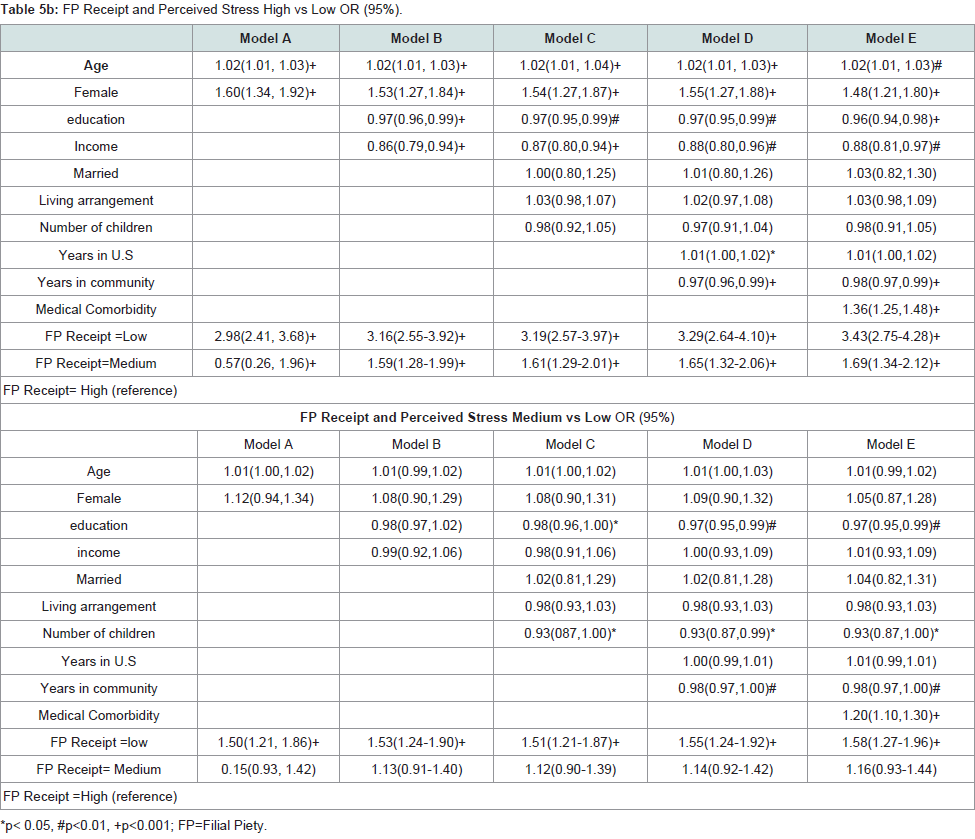
Table 5b: FP Receipt and Perceived Stress High vs Low OR (95%).
Discussion
To our knowledge, this is the first population-based study that reports the associations between filial piety and perceived stress in community-dwelling Chinese older adults. This study demonstrates that lower levels of filial piety receipt are associated with higher levels of perceived stress among Chinese older adults in the greater Chicago area after controlling for potential confounding factors. No significant associations were identified between the expectation of filial piety and perceived stress. Compared with older adults who received a high level of filial piety, older adults who received a medium or a low level of filial piety were more likely to perceive stress as high.Our finding indicates that a low level of filial piety receipt is associated with a high level of perceived stress, providing empirical evidence to support cultural factors impacting health [23]. Our findings are consistent with prior studies suggesting that older adults who receive more emotional support from their closest family members report less symptoms of distress and higher life satisfaction [47,48]. While a majority of previous studies examined the associations between filial piety and care-giving stress targeting caregivers [49,50], our study looks through the lens of older adults to understand the associations between filial piety and perceived stress. The receipt of filial piety may act on stressors in many aspects.
Due to the tradition cultural norms in China which praise the compliance to familial values and disapprove the neglect of filial duties, children being not filial can be a distressed experience for older adults [51,52]. A prior study suggested that cultural factors can shape how stressors are defined, responded, and manifested within a certain population [53]. Despite older adults may suffer from negative feelings of not receiving filial piety, such as shame, disappointment, and embarrassment, a low level of the receipt of filial piety indicate unsatisfactory family relationships and vulnerability to family conflicts [54,55]. It is culturally believed that the presence of disharmony in family relationships disturbs the balance of a person’s everyday life and obstructs the prosperity of the entire family [56]. The tension between family members may be manifested in the form of elder mistreatment [57-65], which in turn may engender more psychological stressors among older adults [24,60,62,66-69].
Moreover, lower levels of filial piety receipt indicate inadequate coping recourses for older adults, letting alone it can function as an intrinsic stressor. Concerning that over one third of Chinese older adults have difficulties in dealing with things in life [37], many Chinese older adults struggle to adjust new lives in the U.S [70-80]. While coping skills and coping resources can both count for stresscoping, coping resources appear to be of higher importance because many uncontrollable factors may impede older adults from acquiring coping skills, such as English proficiency, cognitive functioning, educational level, etc. According to a prior study, older adults perceive coping resources available to be more important for their well-being compared with younger counterparts [81]. Moreover, the benefit of receiving children support is greatly magnified among older adults who attached higher importance towards Chinese familial values [82].
Family support is important for Chinese older adults, but children support may outweigh other forms of family support considering the prevailing trend when large, extended family systems started to divide into nuclear family sectors [82]. Only 9.9% of Chinese older adults denied that they rely on family for support, but as high as 40.4% reported as so with regards to friends [83]. Support from Children is especially important for Chinese older adults in the U.S in terms of dealing with personal situations [38]. Notably, in light of “saving face” as a customary cultural value in China to avoid negative interactions with “outsiders”, older adults who have a low receipt of filial piety may be reluctant to seek other forms of social support.
Our study indicates that the receipt of filial piety, rather than the expectation of filial piety, is significantly associated with perceived stress, which is inconsistent with a prior study showing that the anticipation of social support is a stronger indicator of psychological distress [84]. Our results indicate that older adults with similar levels of stress tend to be more disparate in filial piety expectations. Many contributors may interfere with the expectation of filial piety among older adults. A previous study took the life-course perspective and explained that the expectation of filial piety is associated with how roles of older parents change within the family [85]. From this perspective, Chinese older parents may lower their expectations of filial piety because they can no longer conform to their culturally anticipated roles as the family leader to provide guidance for children during the course of immigration [86]. Culturally, higher levels of expectation of filial piety are built on the presumption that older parents possess greater wisdom and social resources contributing to the prosperity of children. Reciprocally, they deserve filial piety from children in late life. However, this mutual exchange of support between parents and children is often deteriorated with the process of immigrating to U.S, when many of older adults cannot keep up pace with their children in terms of language proficiency and cultural adaptability etc.
Moreover, a greater expectation of filial piety is often predisposed to an explicit expression of the weakness and vulnerabilities among older adults. While many older adults received public elder care from the U.S social welfare, they may be pressured to lower their expectations of filial piety since their practical needs are fulfilled. However, public elder care cannot substitute for the practice of filial piety since filial piety is more than providing support in everyday functioning, but also enhancing inter-generational interactions and parent-children relationships. A prior study contended that older adults with stronger belief in filial piety would prefer kinship over the public elder care [87]. Our study calls for a better understanding on contributing factors that are associated with expectations of filial piety.
Our findings may contribute to existing literature in the following aspects. First, to our best knowledge, this is the first study that quantifies the association between the receipt of filial piety and perceived stress among Chinese older adults. Despite prior studies identified that filial piety significantly contributes to the well-being of Chinese older adults, few has delineated the specific association between filial piety and perceived stress, an important health measure of psychological well-being. Second, our study distinguished the expectation and the receipt of filial piety, and assessed their associations with perceived stress separately. Our results revealed that filial piety expectation and receipt are not congruent in terms of their associations with perceived stress [32]. Further research is needed to explain the reason why only the filial piety receipt is associated with perceived stress.
Third, considering that culturally-relevant frameworks are still wanting in most current studies of successful aging [88], our findings point to the need of initiating a theoretical conceptual framework, in which integral cultural values, such as filial piety, can be incorporated in the assessment of the perceived stress among minority agingpopulations. Fourth, our recruitment was largely benefited from community-based participatory research (CBPR) approach and mixed outreach strategies. Our research assistants are bicultural and bilingual, well-trained to proficiently carry out interviews with older adults in participants’ preferred languages and dialects. During the in-person interviews, older adults can comfortably share their opinions and experiences given that research assistants are equipped with cultural competencies to minimize cultural barriers and stigma that are associated with reporting psychological distress [66].
Limitations of our study warrant mention. First, it is inconclusive whether or not our findings can be generalized to other Chinese populations in the U.S or in Asian societies, although this study was representative of Chinese older adults in the greater Chicago area. Second, our measures of perceived stress and filial piety were subjective, which may be biased in revealing the actual stress levels and actual receipt of filial piety. Third, since we asked participants to make an overall estimate of filial piety receipt from all of their children, we were not able to identify the variations of each child in performing piety duties. Fourth, we used the aggregate score to estimate the overall filial piety expectation and receipt, and therefore whether each filial behavior is associated with perceived stress is not clear. Fifth, the cross-sectional design cannot suggest causal relationship and future longitudinal study is necessary to provide better understanding on associations found in this study.
This research has wide implications for researchers, healthcare professionals, community organizations, and policy makers. First, this study calls for more research attention to explore how cultural values and norms may influence the psychological well-being of minority aging populations. A better understanding on the underlying mechanism through which filial piety receipt influences perceived stress is necessary as it will help develop targeted stress coping strategies for Chinese older adults. Moreover, in-depth analyses can be conducted to specify which domain(s) of the filial piety receipt may contribute to higher perceived stress, as each domain of filial piety can influence perceived stress differently. Second, U.S healthcare professionals need to understand the cultural significance of filial piety. While filial piety is a measure of family relationship, it should be also considered as an important indicator for psychological well-being of Chinese older adults. Health professionals should understand health risks associated with not receiving enough filial piety among Chinese older adults when delivering medical services.
Third, while filial therapy is widely used to increase parentalchildren interactions for young parents in recent studies, its adoption in programs for adult children and older parents is rare. Workshops and education opportunities should be created to encourage older parents and their adult children in sharing their opinions on filial care. Community organizations should involve in family members, especially adult children, when developing stress alleviation programs for older adults. Moreover, programs should also consider remove logistic barriers that may inhibit adult children from engaging in filial piety activities, filial duties can be performed through innovative channels including emails, phones, mobile chatting applications, etc.Fourth, policy-makers should increase Chinese older adults’ access to stress coping resources in the community with language and culture sensitivity in the minority communities. Also, trainings can be provided to adult children to prepare them better in providing elder care to older parents.
Conclusion
In summary, our study found that lower levels of filial piety receipt were associated with higher levels of perceived stress among U.S Chinese older adults in the Greater Chicago area. However, filial piety expectation was not significantly associated with perceived stress. Our study points to the need of incorporating cultural factors into the investigation of perceived stress. Future longitudinal studies are needed to better explain the associations found in this study.Acknowledgements
Funding informationDr. Dong was supported by National Institute on Aging grant (R01AG042318, R01 MD006173, R01 CA163830, R34MH100443, R34MH100393, P20CA165588, R24MD001650 & RC4 AG039085), Paul B. Beeson Award in Aging, The Starr Foundation, American Federation for Aging Research, John A. Hartford Foundation and The Atlantic Philanthropies.
References
- Lazarus RS, Folkman S (1984) Stress, appraisal, and coping. Springer Publishing Company, Inc, New York.
- Laugero KD, Falcon LM, Tucker KL (2011) Relationship between perceived stress and dietary and activity patterns in older adults participating in the Boston Puerto Rican Health Study. Appetite 56: 194-204.
- Henderson KM, Clark CJ, Lewis TT, Aggarwal NT, Beck T, et al. (2013) Psychosocial distress and stroke risk in older adults. Stroke 44: 367-372.
- Aggarwal NT, Clark CJ, Beck TL, Mendes de Leon CF, DeCarli C, et al. (2014) Perceived stress is associated with subclinical cerebrovascular disease in older adults. Am J Geriatr Psychiatry 22: 53-62.
- Rice PL (1999) Stress and health. Brooks/Cole Publishing, Pacific Grove, CA.
- Neupert SD, Almeida DM, Charles ST (2007) Age differences in reactivity to daily stressors: the role of personal control. J Gerontol B Psychol Sci Soc Sci 62: P216-P225.
- Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G (2004) Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci 59: 255-263.
- Schulz JH (2001) The economics of aging: ABC-CLIO.
- Yun RJ, Lachman ME (2006) Perceptions of aging in two cultures: Korean and American views on old age. J Cross Cult Gerontol 21: 55-70.
- Ron P (2007) Elderly people's attitudes and perceptions of aging and old age: the role of cognitive dissonance? Int J Geriatr Psychiatry 22: 656-662.
- Rodin J (1980) Managing the stress of aging: The role of control and coping. In: Coping and health. Springer, pp. 171-202.
- Spielberger CD (2013) Anxiety: Current trends in theory and research, Volume II. Academic Press, New York.
- Kiyak HA, Hooyman NR (1994) Minority and socioeconomic status: Impact on quality of life in aging. In: Abeles RP, Gift HC, Ory MG, (Eds). Aging and quality of life. Springer Publishing Company, New York, pp. 295-315.
- Treas J, Mazumdar S (2002) Older people in America's immigrant families: dilemmas of dependence, integration, and isolation. J Aging Stud 16: 243-258.
- Sanders JM, Nee V (1996) Immigrant self-employment: The family as social capital and the value of human capital. Am Sociol Rev 2: 231-249.
- Ku L, Matani S (2001) Left out: immigrants’ access to health care and insurance. Health Aff (Millwood) 20: 247-256.
- Ponce NA, Hays RD, Cunningham WE (2006) Linguistic dis parities in health care access and health status among older adults. J Gen Intern Med 21: 786-791.
- Gany FM, Herrera AP, Avallone M, Changrani J (2006) Attitudes, knowledge, and health-seeking behaviors of five immigrant minority communities in the prevention and screening of cancer: a focus group approach. Ethn Health 11: 19-39.
- Kim YJ (2009) Comparison of health habits, perceived stress, depression, and suicidal thinking by gender between elders living alone and those living with others. J Korean Acad Fundam Nurs 16: 333-344.
- Folkman S, Lazarus RS, Pimley S, Novacek J (1987) Age differences in stress and coping processes. Psychol Aging 2: 171-184.
- Baum A, Garofalo JP, Yali AM (1999) Socioeconomic status and chronic stress. Does stress account for SES effects on health? Ann N Y Acad Sci 896: 131-144.
- Matud MP (2004) Gender differences in stress and coping styles. Pers Individ Dif 37: 1401-1415.
- Jackson JS, Antonucci TC, Gibson RC (1990) Cultural, racial, and ethnic minority influences on aging. In: barren JE, Schaie KW (Eds). Handbook of the psychology of aging. Academic Press, New York, pp. 3: 103-123.
- Dong X, Chang ES, Zeng P, Simon MA (2015) Suicide in the global Chinese aging population: a review of risk and protective factors, consequences, and interventions. Aging Dis 6: 121-130.
- 25. Tseng WS, Wu DY (2013) Chinese culture and mental health. Academic Press, Inc, New York.
- Marsella AJ, Yamada AM (2000) Culture and mental health: an introduction and overview of foundations, concepts, and issues.
- Hoeffel EM, Rastogi S, Kim MO, Shahid H (2012) The Asian population: 2010. US Department of Commerce, Economics and Statistics Administration, US Census Bureau.
- United States Census Bureau (2010) American community survey.
- Ikels C (2004) Filial piety: practice and discourse in contemporary East Asia. Stanford University Press, California.
- Lan PC (2002) Subcontracting filial piety elder care in ethnic Chinese immigrant families in California. J Fam Issues 23: 812-835.
- Ng AC, Phillips DR, Lee WK (2002) Persistence and challenges to filial piety and informal support of older persons in a modern Chinese society: a case study in Tuen Mun, Hong Kong. J Aging Stud 16: 135-153.
- Dong X, Chang ES, Wong E, Simon M (2012) A qualitative study of filial piety among community dwelling, Chinese, older adults: changing meaning and impact on health and well-being. J Intergener Relatsh 10: 131-146.
- Liu JH, Ng SH, Weatherall A, Loong C (2000) Filial piety, acculturation, and intergenerational communication among New Zealand Chinese. Basic Appl Soc Psych 22: 213-223.
- Liu JH, Ng SH, Weatherall A, Loong C (2000) Filial piety, acculturation, and intergenerational communication among New Zealand Chinese. Basic Appl Soc Psych 22: 213-223.
- Zhan HJ (2004) Willingness and expectations: Intergenerational differences in attitudes toward filial responsibility in China. Marriage Fam Rev 36: 175-200.
- Yu LC (1983) Patterns of filial belief and behavior within the contemporary Chinese American family. Int J Sociol Fam 13: 17-36.
- Zhang M, Simon MA, Dong X (2014) The prevalence of perceived stress among US Chinese older adults. AIMS Med Sci 1: 40-56.
- Wong ST, Yoo GJ, Stewart AL (2005) Examining the types of social support and the actual sources of support in older Chinese and Korean immigrants. Int J Aging Hum Dev 61: 105-121.
- Dong X, Wong E, Simon MA (2014) Study design and implementation of the PINE study. J Aging Health 26: 1085-1099.
- Dong X, Chang ES, Wong E, Simon M (2011) Working with culture: lessons learned from a community-engaged project in a Chinese aging population. Aging Health 7: 529-537.
- Dong X, Li Y, Chen R, Chang ES, Simon M (2013) Evaluation of community health education workshops among Chinese older adults in Chicago: a community-based participatory research approach. J Educ Train Stud 1: 170-181.
- Simon MA, Chang ES, Rajan KB, Welch MJ, Dong X (2014) Demographic characteristics of U.S. Chinese older adults in the Greater Chicago area: assessing the representativeness of the PINE Study. J Aging Health 26: 1100-1115.
- Cohen S, Kamarck T, Mermelstein R (1983) A global measure of perceived stress. J Health Soc Behav 24: 385-396.
- Cohen S, Wills TA (1985) Stress, social support, and the buffering hypothesis. Psychol Bull 98: 310-357.
- Chang ES, Beck T, Simon MA, Dong X (2014) A psychometric assessment of the psychological and social well-being indicators in the PINE study. J Aging Health 26: 1116-1136.
- Gallois C, Giles H, Ota H, Pierson HD, Ng SH, et al. (1999) Intergenerational communication across the Pacific Rim: an initial eight-nation study. The impact of filial piety. In: Latest contribution to cross-cultural psychology. Swets & Zeitlinger, Lisse, Netherlands.
- Leung KK, Chen CY, Lue BH, Hsu ST (2007) Social support and family functioning on psychological symptoms in elderly Chinese. Arch Gerontol Geriatr 44: 203-213.
- Yeung GT, Fung HH (2007) Social support and life satisfaction among Hong Kong Chinese older adults: family first? Eur J Ageing 4: 219-227.
- Lai DW (2010) Filial piety, caregiving appraisal, and caregiving burden. Res Aging 32: 200-223.
- Knight BG, Sayegh P (2010) Cultural values and caregiving: the updated sociocultural stress and coping model. J Gerontol B Psychol Sci Soc Sci 65B: 5-13.
- Keller S (2006) Four theories of filial duty. Philos Q 56: 254-274.
- Sommers CH (1986) Filial morality. J Philos 83: 439-456.
- Krause N, Liang J (1993) Stress, social support, and psychological distress among the Chinese elderly. J Gerontol 48: P282-P291.
- Yeh KH, Bedford O (2004) Filial belief and parent-child conflict. Int J Psychol 39: 132-144.
- Kwan KL (2000) Counseling Chinese peoples: perspectives of filial piety. Asian J Couns 7: 23-41.
- Dilworth-Anderson P, Gibson BE (2002) The cultural influence of values, norms, meanings, and perceptions in understanding dementia in ethnic minorities. Alzheimer Dis Assoc Disord Suppl 16: S56-S63.
- Pillemer KA, Wolf RS (1986) Elder abuse: conflict in the family. Greenwood Publishing Group.
- Wolf RS, Pillemer KA (1989) Helping elderly victims: the reality of elder abuse: Columbia University Press, New York.
- Dong X, Chen R, Chang ES, Simon M (2013) Elder abuse and psychological well-being: a systematic review and implications for research and policy--a mini review. Gerontology 59: 132-142.
- Dong X, Chang ES, Wong E, Wong B, Simon MA (2011) How do U.S. Chinese older adults view elder mistreatment?: findings from a community-based participatory research study. J Aging Health 23: 289-312.
- Dong X, Simon MA, Gorbien M (2007) Elder abuse and neglect in an urban Chinese population. J Elder Abuse Negl 19: 79-96.
- Dong X, Simon M (2015) Prevalence of elder self‐neglect in a Chicago Chinese population: the role of cognitive physical and mental health. Geriatr Gerontol Int. [Epub ahead of print].
- Dong X (2016) Sociodemographic and socioeconomic characteristics of elder self-neglect in an US Chinese aging population. Arch Gerontol Geriatr 64: 82-89.
- Dong X, Chen R, Fulmer T, Simon MA (2014) Prevalence and correlates of elder mistreatment in a community-dwelling population of U.S. Chinese older adults. J Aging Health 26: 1209-1224.
- Dong X, Chen R, Simon MA (2014) Anxiety among community-dwelling U.S. Chinese older adults. J Gerontol A Biol Sci Med Sci 69: S61-S67.
- Dong X, Simon MA (2013) Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med 173: 911-917.
- Dong X, Chen R, Wu B, Zhang NJ, Mui AC, et al. (2015) Association between elder mistreatment and suicidal ideation among community-dwelling Chinese older adults in the USA. Gerontology 62: 71-80.
- Dong XQ (2015) Elder abuse: systematic review and implications for practice. J Am Geriatr Soc 63: 1214-1238.
- Dong X (2015) Elder abuse in Chinese populations: a global review. J Elder Abuse Negl 27: 196-232.
- Mui AC, Kang SY (2006) Acculturation stress and depression among Asian immigrant elders. Soc Work 51: 243-255.
- Dong X, Zhang M, Simon M (2014) The prevalence of cardiopulmonary symptoms among Chinese older adults in the Greater Chicago area. J Gerontol A Biol Sci Med Sci 69 Suppl 2: S39-S45.
- Simon MA, Chang ES, Zhang M, Ruan J, Dong X (2014) The prevalence of loneliness among U.S. Chinese older adults. J Aging Health 26: 1172-1188.
- Dong X, Zhang M, Simon MA (2014) Self-mastery among Chinese older adults in the Greater Chicago area. AIMS Med Sci 1: 57-72.
- Dong X, Chen R, Simon MA (2014) Experience of discrimination among U.S. Chinese older adults. J Gerontol A Biol Sci Med Sci 69 Suppl 2: S76-S81.
- Dong X, Zhang M (2015) Religiosity among U.S. Chinese older adults in the Greater Chicago area-findings from the PINE Study. J Relig Spiritual Aging 27: 323-342.
- Simon MA, Zhang M, Dong X (2014) Trust in physicians among U.S. Chinese older adults. J Gerontol A Biol Sci Med Sci 69 Suppl 2: S46-S53.
- Dong X, Bergren SM, Chang ES (2015) Levels of acculturation of Chinese older adults in the Greater Chicago area - The population study of Chinese elderly in Chicago. J Am Geriatr Soc 63: 1931-1937.
- Chen R, Dong X (2015) The Prevalence and correlates of gambling participation among community-dwelling Chinese older adults in the U.S 2: 90-103.
- Chen R, Simon MA, Dong X (2014) Gender differences in depressive symptoms in U.S. Chinese older adults. AIMS Med Sci 1: 13-27.
- Dong X, Chang ES, Simon MA (2014) Physical function assessment in a community-dwelling population of U.S. Chinese older adults. J Gerontol A Biol Sci Med Sci 69 Suppl 2: S31-S38.
- Hamarat E, Thompson D, Zabrucky KM, Steele D, Matheny KB, et al. (2001) Perceived stress and coping resource availability as predictors of life satisfaction in young, middle-aged, and older adults. Exp Aging Res 27: 181-196.
- Chen X, Silverstein M (2000) Intergenerational social support and the psychological well-being of older parents in China. Res Aging 22: 43-65.
- Chen R, Simon MA, Chang ES, Zhen Y, Dong X (2014) The perception of social support among U.S. Chinese older adults findings from the PINE study. J Aging Health 26: 1137-1154.
- Krause N (1997) Anticipated support, received support, and economic stress among older adults. J Gerontol B Psychol Sci Soc Sci 52: P284-P293.
- Sheng X, Settles BH (2006) Intergenerational relationships and elderly care in China a global perspective. Curr Sociol 54: 293-313.
- George LK (1989) Stress, social support, and depression over the life-course. In: Markides KS, Cooper CL, (Eds). Aging, stress and health. John Wiley & Sons, Oxford, England, pp. 241-267.
- Cheung CK, Kwan AY, Ng SH (2006) Impacts of filial piety on preference for kinship versus public care. J Community Psychol 34: 617-634.
- Torres S (1999) A culturally-relevant theoretical framework for the study of successful ageing. Ageing Soc 19: 33-51.
are worded in a positive direction, so they were