
Journal of Oral Biology
Download PDF
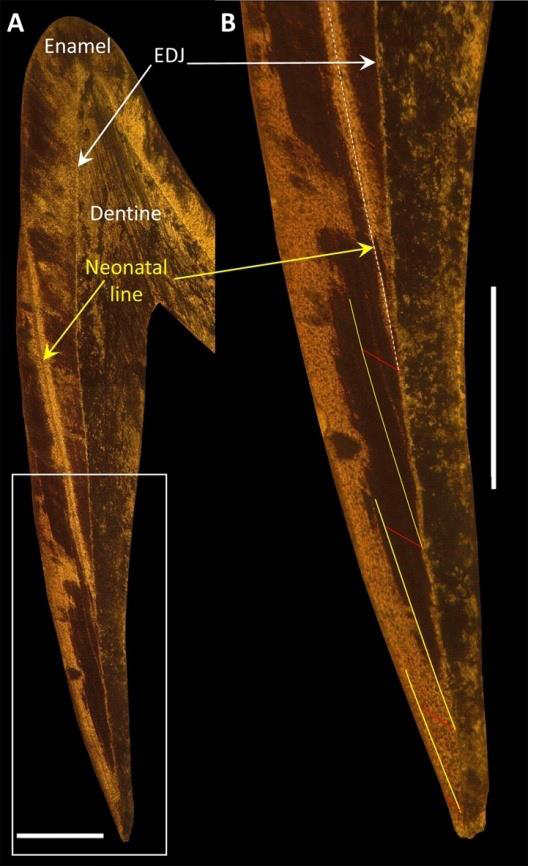 Figure 1: A.Thin section of the 268a tooth. The neonatal line (NNL) is
clearly visible. B. Detail of the enamel close to the cervix showing the method
usedto estimate age at death. Every 100 μm along the prism length (in red)
corresponds to 30 days. Successive stages in enamel formation starting at the
NNL are shown by striae of Retzius (yellow lines). In total, three successive
100 μm lengths and an additional prism length of 48 μm suggest anage at
death of 3.2 months. EDJ: enamel-dentine junction. The bar corresponds to
500 μm.
Figure 1: A.Thin section of the 268a tooth. The neonatal line (NNL) is
clearly visible. B. Detail of the enamel close to the cervix showing the method
usedto estimate age at death. Every 100 μm along the prism length (in red)
corresponds to 30 days. Successive stages in enamel formation starting at the
NNL are shown by striae of Retzius (yellow lines). In total, three successive
100 μm lengths and an additional prism length of 48 μm suggest anage at
death of 3.2 months. EDJ: enamel-dentine junction. The bar corresponds to
500 μm.
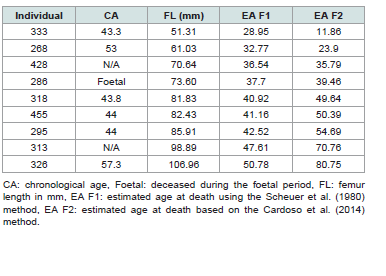 Table 1:Chronological ages and ages at death in weeks estimated from femur length
Table 1:Chronological ages and ages at death in weeks estimated from femur length
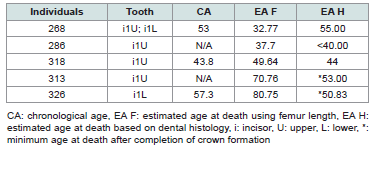 Table 2:Chronological ages and estimated ages at death in weeks
Table 2:Chronological ages and estimated ages at death in weeks
 Figure 2:Comparison of documented chronological ages with estimated
ages at death from femur length. CA: chronological age; EA F1: estimated
age at death using the Scheuer et al. (1980) method; EA F2: estimated age at
death using the Cardoso et al. (2014) equation.
Figure 2:Comparison of documented chronological ages with estimated
ages at death from femur length. CA: chronological age; EA F1: estimated
age at death using the Scheuer et al. (1980) method; EA F2: estimated age at
death using the Cardoso et al. (2014) equation.
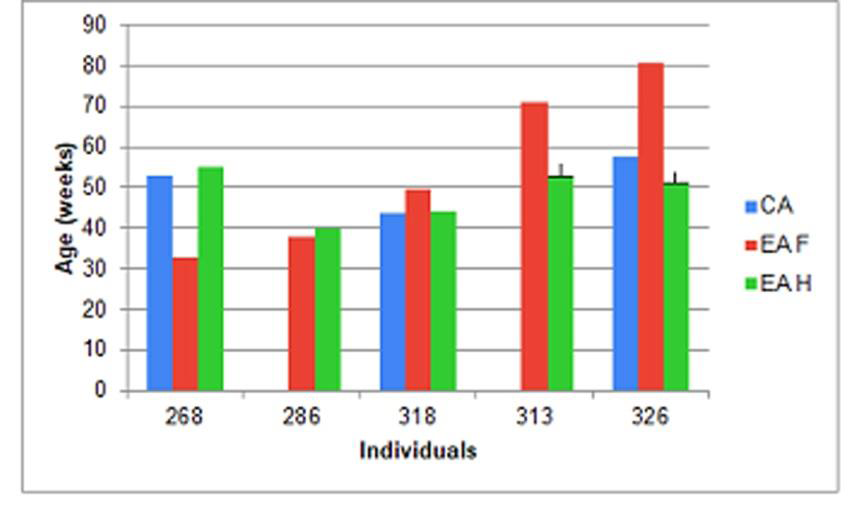 Figure 3:Comparison of documented chronological ages with estimated ages
at death from femur length and dental histology. CA: chronological age, EA F:
estimated age at death from femur length using the two methods combined
for prenatal and postnatal individuals, EA H: estimated age at death from
dental histology analysis. ┴: Individuals 313 and 326 have full crown and root
formation so that dental histology gives a minimum age.
Figure 3:Comparison of documented chronological ages with estimated ages
at death from femur length and dental histology. CA: chronological age, EA F:
estimated age at death from femur length using the two methods combined
for prenatal and postnatal individuals, EA H: estimated age at death from
dental histology analysis. ┴: Individuals 313 and 326 have full crown and root
formation so that dental histology gives a minimum age.
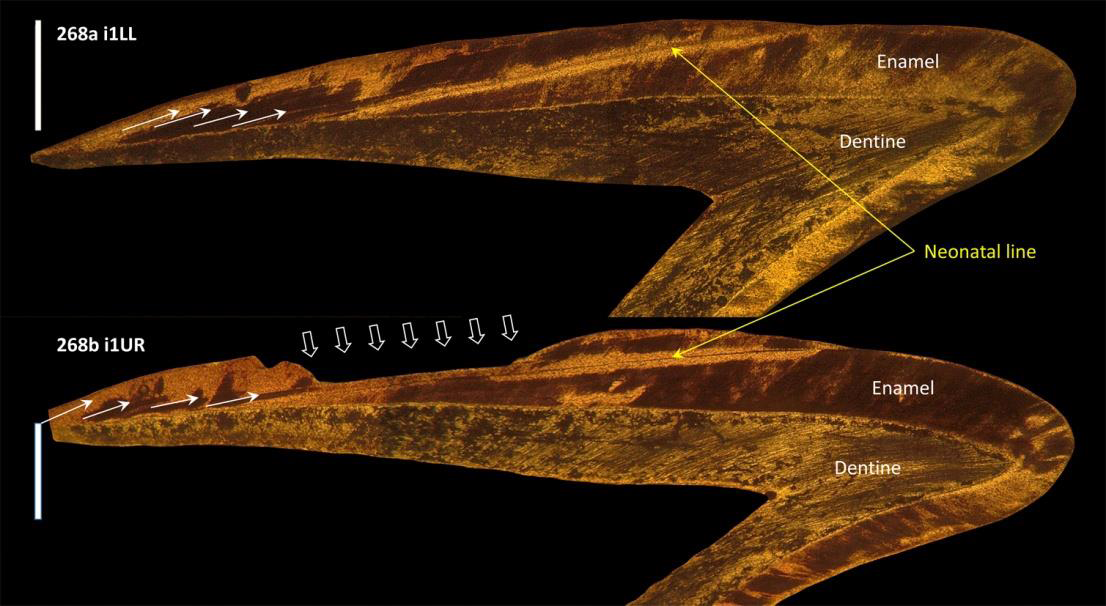 Figure 4:These two teeth from the same individual (268a, 268b) show
accentuated striae (white arrows) in the postnatal enamel. These stress
marks are more marked in the upper right incisor (268b) where ameloblasts
precociously interrupted enamel secretion, producing a hypoplasia in the
central area of the crown’s buccal face (broad white arrows). i1LL: lower
left first deciduous incisor, i1UR: upper right first deciduous incisor. The bar
corresponds to 500 μm.
Figure 4:These two teeth from the same individual (268a, 268b) show
accentuated striae (white arrows) in the postnatal enamel. These stress
marks are more marked in the upper right incisor (268b) where ameloblasts
precociously interrupted enamel secretion, producing a hypoplasia in the
central area of the crown’s buccal face (broad white arrows). i1LL: lower
left first deciduous incisor, i1UR: upper right first deciduous incisor. The bar
corresponds to 500 μm.
Research Article
Assessment of Age at Death in Perinatal Individuals from Dental Histology Analysis. An Exploratory Study
Ramirez Rozzi F1,2*, Petrone S3,4, Plischuk M3, Desántolo B3 and Mancuso RG3
1UMR 7206 Ecoanthropologie, MNHN-CNRS-UPCité, Musée de
l’Homme, Paris, France
2UMR 1333 Oral Health, UPCité, INSERM, Montrouge, France
3LICIF, Facultad de Ciencias Médicas, UNLP, La Plata, Argentina
4Ministerio de Salud de la Provincia de Buenos Aires, Argentina
2UMR 1333 Oral Health, UPCité, INSERM, Montrouge, France
3LICIF, Facultad de Ciencias Médicas, UNLP, La Plata, Argentina
4Ministerio de Salud de la Provincia de Buenos Aires, Argentina
*Address for Correspondence:Fernando Ramírez Rozzi, UMR 7206
Ecoanthropologie, MNHN-CNRS-UPCité, Musée de l’Homme, Paris, France.
E-mail Id: fernando.ramirez-rozzi@mnhn.fr
Submission:08 January 2025
Accepted:30 January 2025
Published:31 January 2025
Copyright: © 2025 Ramirez Rozzi F, et al. This is an open access
article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Keywords:Chronological Age; Enamel; Incremental Lines; Striae of Retzius;
Neonatal Line; Femur Length
Abstract
Age estimation is one of the main data used in the study of child
skeletal remains in forensic and bioarchaeological investigations.
Objective: Our aim was to assess the age at death attributed through methods based on bone development and by analysing the microstructure of tooth enamel.
Methods: Age at death was estimated using femur length and dental histology in 9 perinatal individuals of known age. Two methods were selected for the estimation of age at death from femur length. Previous work has reported that these two methods produce the best estimations of the age at death of individuals. For the dental histology analysis, longitudinal ground sections of 6 deciduous incisors from 5 individuals were examined. Incremental lines in the tooth enamel (striae of Retzius and the neonatal line) were used to estimate the age at death, assuming a daily secretion rate of 3.23 μm.
Results: The ages estimated by the two methods based on femur length differ, except for those concerning the last stage of gestation. It is interesting to note that the accuracy of the estimation depends on whether the method was established with prenatal or postnatal individuals. Estimated ages based on dental histology (N=3 individuals) are consistent with the recorded data.
Conclusion: The study of dental histology based on the analysis of enamel microanatomy has some limitations but allows the age at death in to be established very accurately. The quality and quantity of data that this technique provides is of prime importance for forensic studies and for analyses of historical populations and archaeological remains.
Objective: Our aim was to assess the age at death attributed through methods based on bone development and by analysing the microstructure of tooth enamel.
Methods: Age at death was estimated using femur length and dental histology in 9 perinatal individuals of known age. Two methods were selected for the estimation of age at death from femur length. Previous work has reported that these two methods produce the best estimations of the age at death of individuals. For the dental histology analysis, longitudinal ground sections of 6 deciduous incisors from 5 individuals were examined. Incremental lines in the tooth enamel (striae of Retzius and the neonatal line) were used to estimate the age at death, assuming a daily secretion rate of 3.23 μm.
Results: The ages estimated by the two methods based on femur length differ, except for those concerning the last stage of gestation. It is interesting to note that the accuracy of the estimation depends on whether the method was established with prenatal or postnatal individuals. Estimated ages based on dental histology (N=3 individuals) are consistent with the recorded data.
Conclusion: The study of dental histology based on the analysis of enamel microanatomy has some limitations but allows the age at death in to be established very accurately. The quality and quantity of data that this technique provides is of prime importance for forensic studies and for analyses of historical populations and archaeological remains.
Introduction
Estimated age at death is one of the main data used in the study of
child skeletal remains in forensic and bioarchaeological investigations
[1,2]. Age data are fundamental in building up individual biological
profiles, which contributes to the judicial system and has legal
implications in forensic cases [3,4] as well as allowing reconstructions
of mortality profiles and interpretations of the impact of changes
in the lifestyle of past populations [5]. Furthermore, with accurate
estimations of gestational and post-gestational age, this variable can
be associated with factors that may have modified the normal growth
trajectory [6].
The gradual changes that occur during growth and development
are used as indicators to estimate age. Tooth formation, dental
eruption and long bone development are the preferred anatomical
references for establishing growth patterns in foetal, perinatal and
infant individuals. These patterns are established from the analysis of
individuals of known age and are used as a reference to estimate age
in cases where it is unknown [7,3].
An enormous amount of data from long bone growth surveys
has been used to develop regression equations for age estimation.
It should be noted that some equations were developed to estimate
gestational age in the prenatal period [8-10]. While others were
proposed for the postnatal period [11-13]. There are many clinical
studies on the gestational age of preterm infants and small babies that
assess health, growth and development. However, these groups are
impossible to identify when assessing the remains of long bones of
foetuses and infants from archaeological sites [13]. Unfortunately,
there is no method for estimating age using long bones that takes
the pre-postnatal continuum into account [13]. This observation is
important because the origin and characteristics of the samples from
which the estimation methods are developed influence the results
and interpretations when they are extrapolated to other samples or
populations [14-17].
A method that allows age to be obtained directly, with
inbuilt chronological identification, would avoid the problems of
extrapolation. Dental histology studies can fulfil this purpose because
they are based on the presence of growth lines in the enamel whose
analysis in deciduous teeth can be used to identify premature births
and estimate the age at death of infant individuals. These growth lines
can therefore provide a precise chronology of the formation of the
tooth [18-21] as well as the age at death if the tooth was not fully formed
[22-25]. The enamel has two types of growth lines: cross-striations
and striae of Retzius. The former, which are perpendicular to the axis
of the prisms, result from the circadian activity of ameloblasts, so that
each cross-striation corresponds to one day [26]. The striae of Retzius
are arranged obliquely to the axis of the prisms and correspond to
successive increments in the formation of the enamel matrix. Striae
of Retzius have a regular systemic periodicity that can vary from
tooth to tooth for about 6-9 days. Each stria corresponds to a specific
moment of tooth formation and highlights the active ameloblasts at
that moment. The etiology of the striae is unknown but they are the
result of physiological, natural changes. Moments of stress produce
accentuated striae [20], sometimes they are identifiable on the surface
of the tooth as hypoplasias.
Birth is a time of stress, and is manifested in tooth enamel by
a very marked stria known as the neonatal line (NNL) [27,28].
The link between NNL and birth can be observed in the difference
between birth conditions. For instance, NNL virtually does not exist
in stillbirth cases and NNL thickness is thicker after vaginal delivery
than after caesarean section [29] which is used as an argument in
favor of caesarean section being less stressful for the newborn [30].
Birth is easily identifiable in temporary teeth because their formation
begins in utero and ends in early childhood. The NNL thus calibrates
all temporary teeth and distinguishes between prenatal and postnatal
enamel. In addition, given the stress sensitivity of striae, periods of
childhood stress can be identified post-mortem through the presence
of strongly marked lines formed after the NNL. Preliminary evidence
suggested that deprivation or threat (physical and sexual abuse,
neglect, trauma) may present themselves as stress lines in the enamel
[31]. There are various potential causes of stress, such as infections,
high fevers or periods of starvation. In addition, depending on the
location of the NNL in the crown, it is possible to infer whether
the birth occurred at term (location of the NNL similar to control
individuals) or prematurely, in which case the NNL is closer to the
dentin horn. Thus, the study of the micro-anatomy of the enamel
in deciduous teeth not only provides a) the chronology of crown
formation, but also b) calibrates it with birth and therefore c) suggests
an age at death if crown formation was not complete, d) to identify
whether the birth was at term, and e) to characterize the child’s health.
The aim of this exploratory study based on a small sample size
was to show the potential use of enamel microanatomy to suggest an
age at death in immature individuals. To show the limitations of this
analysis teeth whose crown development has ended are also included.
A method based on bone development to suggest an age at death for
the same individuals is presented for comparison.
Material
The individuals studied are from the Lambre collection, which
is composed of skeletons donated by the municipal cemetery of
the city of La Plata (Argentina) to the Faculty of Medical Sciences
of the National University of La Plata for research and teaching
purposes[32,33]. The sex, age, date and cause of death of the human
remains in the collection are documented, but information on the
gestational age of foetal individuals is lacking. The documented death
dates for the children in the collection are between 1927 and 2015.
The individual included in this study died between 1992 and 1997, so
it can be said that the sample is representative of those who died in the
last decade of the twentieth century in La Plata city.
Although there is no specific population characterization for the
individuals of the Lambre collection, the most frequent nationality is
Argentinian, with 58.46% for adults and all sub-adult individuals. The
sample can be described as belonging to an urban and cosmopolitan
population of the Metropolitan Area of Buenos Aires, thus reflecting
a complex demographic history with multiple migration events
and miscegenation events. Genetic studies indicate the presence of
Amerindian, European and African components in proportions of
approximately 14%, 82% and 4% respectively[34,35].
Methods of age estimation based on long bones were applied
to a sample of 9 individuals from the Lambre collection. Of these, 6
individuals have a chronological age (CA) at death in the postnatal
period; 2 individuals do not have documentary information and 1
individual died in the foetal period but no gestational age is available.
Dental histology analysis was performed only for five individuals (268
[i1UR, i1LL], 286, 313, 318, 326). The individual 268 is represented
by two teeth.
The study, conservation, and management of human remains in
this research was in agreement with current national and international
ethic codes. The research on the Lambre collection was approved by
the Bioethics Committee of the Faculty of Medical Sciences of the
National University of La Plata (COBIMED: 0800-013812/12-000).
Methods
Age at death was estimated using femur length (FL) and dental
histology. Two equations were selected for the age estimation from
femur length, one applied to foetal individuals and the other to
postnatal ones. A selection was necessary because the individuals in
the sample are pre- and postnatal in age and there are no age estimation
equations covering both periods together. These two equations were
chosen because they proved to give the most accurate results for
estimating age in individuals up to one postnatal year in the Lambre
collection [15]. [8] [FL * 0.3922) + 8.83] is the most appropriate
equation for foetal individuals, and [13]. [(FL - 74.04)/42.01] for
postnatal individuals. Age is given in weeks from conception and
birth is assumed to have occurred at week 40 of gestation.
These equations produce a bias when used in individuals of
other ages [8] (the Scheuer et alequation in postnatal cases and the
Cardoso et al equation one in prenatal cases) (see Results). For this
reason, in order to compare the age that was estimated according to
the length of the femur with the age obtained from dental histology,
the equation to be applied depended on whether the individual is preor
postnatal, considering a femur length of 79 mm as the boundary
between the pre- and post-natal periods [9,36]. In other words, the
[8] equation was used for individuals with a shorter femur length, and
[13] equation for those with longer femurs, so that the results could
be compared with those from the dental histology analysis.
For the analysis based on dental histology, the teeth were
sectioned using the methodology described in [37]. The age at death
was estimated using the method described by [38,39]. The NNL was
identified in each tooth section [Figure 1]. The point of intersection
of the NNL with the enamel-dentine junction (EDJ) was used as a
starting point. In the prism placed at this intersection, a point was
established at 100 μm from the EDJ. The stria of Retzius passing
through this point was followed to its intersection with the EDJ. This
triangle corresponds to one area of the enamel. The same procedure
was performed up to the dentin horn and to the cervix to establish
several areas of prenatal and postnatal enamel. [38] found an average
of 3.23 μm for deciduous canines, established from 559 measurements
of the daily secretion rate in the enamel 100 μm from the EDJ. They
proposed that each area of enamel is therefore formed in 30 days. To
obtain the age at death after birth, the number of areas of post-natal
enamel in each section was multiplied by 30 and the length of prism
formed after the last area of enamel was divided by 3.23 to add the last
days of enamel formation.
The sections were observed with a Leica M8 stereo microscope
and a Zeiss Universal transmitted and polarized light optical
microscope using x2.5, x6.3 and x16 lenses. The digital images were
acquired using an adaptable IDEA® removable camera placed on
the eyepiece of the optical microscope and captured on a computer
using Spotbasic®software. The images were processed with Nikon
ViewNX2® for contrast enhancement and adjustments, ImageJ® (Fiji)
for line tracing and data acquisition, and Adobe Photoshop® for
photo editing
Results
The chronological age and the age estimated from femur length
are presented in [Table 1]. The estimated ages of individuals 333 and
268 from femur length are very low relative to the chronological ages
[Figure 2]. This could indicate that these are premature individuals.
According to their femur length, individuals 428 and 286 were in the
last stage of gestation: both equations based on femur length yield
similar results for these individuals. It is interesting to note that
the ages estimated by the [8] method, based on foetal individuals,
underestimates the ages of postnatal individuals (318, 455, 295, 313,
326) and, conversely, the ages estimated by [13] whose equation is
based on postnatal individuals, underestimates the ages of foetal
individuals (333, 268).
The estimated ages based on dental histology (EA H) are given in
[Table 2] . In individuals 268, 286 and 318, crown formation was not
complete, while in the remaining two, 313 and 326, part of the root
was already formed and thus the age at death cannot be provided. In
the four teeth whose crown formation was not complete, the analysis
of dental histology provides very accurate estimations. In 268a and
268b, the age at death is 15 weeks after birth (Figure 3). In tooth
286, the NNL was not observed and in 318, a thin layer of enamel
is posterior to the NNL, suggesting death during the first month
of extra-uterine life. These results are consistent with the cemetery
records [Table 2] ,[Figure 3], which show that 268 died at 53 weeks
(40 weeks gestation and 13 weeks postpartum), 286 died in the foetal
stage (less than 40 weeks) and 318 died27 days (4 weeks) after birth (44 weeks).
In tooth 268a [Figure 1], other marked striae of Retzius can be
observed that formed after the NNL, thus indicating moments of
postnatal stress. Tooth 268b [Figure 4] was even more strongly
affected by stress, since the secretion of ameloblasts was interrupted
at the level of the stress line following the NNL and is responsible for
a significant hypoplasia in the middle crown zone.
The contribution of dental histology based on enamel analysis is
limited in teeth where crown formation is complete. However, the
time between birth and completed crown formation can be known.
This is important because if the period is longer than usual, it can
be inferred that the birth was premature. In 313 and 326, the time
between birth and the end of crown formation is 3 and 2.5 months
respectively (13 and 10.83 weeks), indicating that the birth was not
premature. To obtain the age at death in these latter cases, the analysis
should include dentine. Unfortunately, growth lines in this tissue are
not easy to discern and observations can rarely be made. In cases
where root formation has begun, an estimate based on dental metrics
can be used [40,41] but this was outside the scope of our study.
Discussion
Several methods based on bone growth have been proposed to
determine the age of foetal, perinatal and infant individuals. These
methods have been established on the basis of surveys of populations
that provide sound information through the biological profiles of
individuals whose chronological age is known. They therefore become
reference methods that are used to estimate ages in individuals whose
biological profiles need to be reconstructed [42]. An extrapolation of
the method was assessed to confirm its applicability to populations
other than the one used to establish it [13,43]. However, the fact that
a method works when extrapolated to a different population does not
ensure that it can be applied to all populations.
In the case of our study, although the individuals analysed are
close in origin to the populations used as a reference (Europeans),
the method based on bone growth (length of the femur) suggests
ages that do not agree with the records. According to this method,
individual 268 died before birth, individual 286 near birth (between
38 and 40 weeks) and individual 318 a few months after birth (Table
1). The bias of these attributions does not follow a similar pattern
either, since the age at death is underestimated for individual 268
and overestimated for individual 318. However, the results from both
equations are consistent when the individuals died in the perinatal
period, as is the case with individuals 286 and 318. This consistency is
confirmed by the dental histology analysis [Table 2].
To estimate age by dental histology, we used a daily rate of
enamel secretion (3.23 microns) determined from the study of an
English population [38]. A close rate (3.26 microns) was obtained in a
population of Baka pygmies [39]. The similarity of these results from
two distantly related populations living in totally different habitats
allowed us to extrapolate the same rate of enamel formation to the
individuals we analysed in this study. The agreement between our
estimates of age at death and the records indicates that the true rate of
enamel formation is no different. If extrapolation has to be avoided,
the daily enamel secretion rate can always be obtained in each
individual under study by measuring the distance between adjacent
cross-striations.
Comparison of chronological age with the two methods used
[Table 2] shows that results from dental histology are closer to
chronological ages than those from the femur length. Age estimations
from femur length were obtained using two equations established
from other population. Bone growth methods yield inconsistent
results when applied to different populations, this limits the use of
this method for comparison and may result in either overestimation
of age or underestimation. Differently the methodology from dental
histology allows to obtain the chronology directly through the
presence of growth lines in the enamel.
However, the method based on the histology of tooth enamel
has its limitations, as we have seen in cases when the formation
of the crown is complete. Once formation of the root has begun,
analysis of the enamel can only determine whether the individual
was born at term but cannot provide the age at death. The growth
lines can be analysed in the dentin, where the lines of Von Ebner and
Andersen correspond to the cross-striations and the striae of Retzius
respectively [44]. However, observation of these lines is much more
difficult except in very exceptional cases.
Another and much more important limitation of dental histology
concerns the availability of the tooth and preparation of the thin
section for analysis. In 4 out of 9 individuals, the dental histology
analysis could not be performed. In the case of individuals 333 and
428 who died in the foetal stage, maturation of the enamel had not
ended and the growth lines are not observable. In individuals 326
and 455, who died after birth, the observation of growth lines and
prisms is of very poor quality, making it impossible to apply the
methodology. This may be accounted for by different factors, such as
biogenetic processes, conservation or preparation.
Analyses of infant mortality need to be addressed by age groups,
since causes of death have different rates and interpretations in
the neonatal and post-neonatal periods. When death is caused by
endogenous factors, such as birth/genetic defects, they are fatal
within a short period after birth. In contrast, exogenous causes such
as infectious diseases and gastrointestinal disorders have a greater
incidence in the post-neonatal period [45]. With improvements in
treatment and care in neonatal care units, there is a higher survival
of premature babies, which has changed the epidemiology of infant
mortality. However, premature birth and low birth weight are still
variables associated with a higher risk of death [46].
The study of dental histology cannot pinpoint the cause of death but
can provide certain indications. In individual 268, the age according
to dental histology coincides with the documented chronological age
but differs from the age that long bone growth would indicate. This
suggests that in this case there may have been a premature birth or
severe restriction of longitudinal growth due to conditions of stress.
In this same individual there are marked striations after the NNL
(Figure 4). This indicates that there were several periods of stress
after birth, one very pronounced which resulted in the formation of
hypoplasia. Although the cause of death in this case is recorded as
non-traumatic cardio-respiratory insufficiency, these signs of stress
indicate that the death of this individual at four months of postnatal
age was the result of a prolonged process and not of an abrupt event.
Conclusion
The study of dental histology based on the analysis of enamel
microanatomy can establish the age at death of neonates. Although
this type of analysis requires an invasive technique and has
limitations that may prevent its application, the precision that can be
obtained could justify its use in many cases. The quality and quantity
of data that this technique provides on the growth and health status
of individuals is of prime importance for forensic studies and for
analyses of historical populations and archaeological remains.
This original research was supported by the CNRS and an excellence prize from the Institut Benjamin Delessert.
This original research was supported by the CNRS and an excellence prize from the Institut Benjamin Delessert.
References
Citation
Ramirez Rozzi F, Petrone S, Plischuk M, Desántolo B, Mancuso RG. Assessment of Age at Death in Perinatal Individuals from Dental Histology Analysis. An Exploratory Study. J Oral Biol. 2025; 9(1): 1.