
Photoreceptor Inner Segment Ellipsoid Band in Diabetic Retinopathy
Sandeep Saxena1, Khushboo Srivastav1, Ross Chod2 and Levent Akduman2*
- 1Retina Service, Department of Ophthalmology, King George’s Medical University, Lucknow, India
- 22Vitreoretinal and Uveitis Service, St. Louis University School of Medicine, Department of Ophthalmology, St. Louis, MO, USA
*Address for Correspondence: Levent Akduman MD, Vitreoretinal and Uveitis Service, St. Louis University School of Medicine, Department of Ophthalmology, St. Louis, MO, USA, E-mail: akdumanlevent@gmail.com
Citation: Saxena S, Srivastav K, Chod R, Akduman L. Photoreceptor Inner Segment Ellipsoid Band in Diabetic Retinopathy. J Ocular Biol. 2015;S(1):5.
Copyright © 2015 Saxena S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Ocular Biology | ISSN: 2334-2838 | Special Issue 1
Submission: 03 November, 2014 | Accepted: 03 January, 2015 | Published: 07 January, 2015
Editors:Dr. Eric M Shrier, Director of Retinal Service and Assistant Professor of Ophthalmology, SUNY Downstate Medical Center, USA
Abstract
Optical coherence tomography (OCT) provides information akin to real-time, in-vivo histology of the retina. Diabetic retinopathy results in structural changes within the retina that can be observed by OCT imaging, and which correlates with the severity of vision loss. Previously, the second most inner highly reflective outer band seen on OCT was believed to represent the junction between the inner and outer segments (the IS/OS junction) of retinal photoreceptors. In addition to macular volume, the extent of inner/outer photoreceptor segment disruption was found to be a reliable predictive factor accounting for visual acuity loss in patients with diabetic retinopathy. More recent reports have actually demonstrated only a weak correlation between central retinal thickness and visual acuity in these patients, implying that vision may be more readily affected by disruption of the microstructural retinal architecture or direct photoreceptor damage. It has since been discovered, however, that the second most inner highly reflective band more accurately corresponds to the microstructural ellipsoid zone of the photoreceptor inner segmentsthat can beseen on retinal histologic analysis. Accurate evaluation of this highly significant microstructural layer can provide valuable information regarding disease state and visual prognosis in diabetic retinopathy and diabetic macular edema. We report on the most current and accepted information regarding this newly re-identified layer and its accurate clinical evaluation.Introduction
The prevalence of diabetes mellitus is attaining epidemic proportions worldwide [1,2]. As of 2013, it is estimated that 382 million people suffer from diabetes mellitus. This number is expected to rise to 592 million by 2035 [3]. Macular edema is the most common cause of vision loss in diabetic retinopathy [4]. Of patients living with diabetes mellitus for a duration of 20 year or more, The Wisconsin Epidemiological Study of Diabetic Retinopathy reported a prevalence of diabetic macular edema of 29% in younger onset diabetics and 28% in older onset diabetics [5].Diabetic retinopathy can result in structural changes within the retina which have been shown to correlate with severity of retinopathy. Optical Coherence Tomography has come to be an exceedingly useful investigative tool for classifying macular edema and quantifying macular thickness in diabetic retinopathy [6-8]. Photoreceptor dysfunction may also be a significant predictor of visual acuity in these patients [9-12]. Inner segment-ellipsoid (ISel) band (previously believed to represent the inner-segment/outersegment, or IS/OS, junction) disruption has been demonstrated to be an important predictor of visual acuity in diabetic macular edema [13]. The integrity of this anatomical microstructural layer appears to be of high clinical importance, as the absence or disruption of this band has been associated with vision loss in a number of other diseases affecting the photoreceptors and/or choroid [14-20]. Accurate evaluation of this bandwilltherefore be of particular interest to the clinicianthat is faced with treating diabetic retinal disease processeson a daily basis. As such, understanding the evaluative parameters of this microstructural layer will be of high clinical importance to the practicing retinal physician.
Anatomy of the Inner Segment Ellipsoid Band
High-resolution spectral domain optical coherence tomography (SD-OCT) provides a nearly cellular level resolution of the retina, invivo. In the foveal region, SD-OCT imaging has conventionally been resolved into four bands. The innermost band has been attributed to the external limiting membrane (ELM), a linear confluence of junctional complexes between Muller cells and photoreceptors [21]. In the past, the second line of high reflectivity has been ascribed to the boundary between the inner segments (IS) and outer segments (OS) of the photoreceptors, often described as the IS/OS junction [22,23]. The third band is commonly referred to as the cone outer segment tips (COST) line, or Verhoeff’s membrane (believed to represent ensheathment of cone outer segments by RPE cell apical processes) [24-26]. The outermost highly-reflective band is believed to represent he retinal pigment epithelium (RPE) itself, although Spaide and Curcio suggest that this fourth band is actually contributed by Bruch’s membrane and the choriocapillaris [27].It has been demonstrated that for foveal cones and rods alike, the length of the IS microstructure is roughly the same as that of the OS microstructure [28-32]. Therefore, one might deduce that the IS/OS junction would form a plane midway between the ELM and RPE, however, in-vivo SD-OCT imaging demonstrates the second reflective band to lie significantly closer to the ELM than to the RPE.
Using ultra high resolution SD-OCT, Fernandez et al. were able to demonstrate the anatomy of human foveal cone photoreceptors, including visualization and identification of the distal inner-segment ellipsoid layer [33]. A scale model drawing of the outer retina was constructed by Spaide and Curcio, which was based on published histology, in order to enable visual comparisons [27]. The conclusion of this analysis on the origin of the first and fourth band was the same as previously suggested.
Anatomical correlation of the second band, however, has been more controversial. By comparative alignment of OCT bands with an anatomically correct model of the outer retina (using freshly isolated living retinas from the leopard frog), Curcio et al. suggest the inner segment ellipsoid layer to be responsible for contributing this secondmost inner highly reflective band [34]. The third band seemed to have originated from the posterior tips of cone outer segments, called the contact cylinders.
When analyzing statistical relationships between visual acuity and macular volume, history of prior treatment, and percent disruption of the second-most inner highly-reflective band seen on OCT, multivariate analysis demonstrated a statistically significant relationship with the latter element [41]. Initial studies found a good correlation between macular thickness, assessed by OCT, and visual acuity [35-38], however, recent reports show only a weak correlation between central retinal thickness and visual acuity in patients with diabetic macular edema (DME) [39]. This might further support the notion of alternative influences more readily impacting visual acuity in these patients, including direct photoreceptor damage and/or disruption of the microstructural retinal architecture (i.e. the inner segment ellipsoid layer) [39,40].
Classification Systems for ISel Disruption
A) Maheshwary et al., obtained horizontal and vertical SD-OCT images through the fovea with scanning laser SD-OCT using either an OPKO-OTI (Toronto, Canada) or a Heidelberg Spectralis (Vista, CA) in sixty-two eyes from 38 patients with diabetic macular edema (DME) [41]. An average foveal thickness value was obtained after reviewing both scans. Next, the photoreceptor IS/OS junction band (now the inner segment ellipsoid layer (ISel) band) was evaluated 500 microns in either direction of the fovea. [ISel] disruption was gradedfrom grade 0–2.• Grade 0: Intact [ISel]
• Grade 1: Focal [ISel] disruption of 200 microns or less in length
• Grade 2: [ISel] disruption greater than 200 microns in length
Grades from each patient’s horizontal and vertical scans were added to yield a global disruption scale. Lastly, the percentage of disruption along the [ISel] band, again measured 500 microns in either direction from the foveal center, was recorded. These percentages were then averaged to generate a number between 0% (no ISel disruption) and 100% (total loss of the ISel band in both horizontal and vertical scans). A statistically significant correlation between percentage of disruption of the [ISel] band and visual acuity was found (P = 0.0312). Additionally, there was a strong trend suggesting a relationship between macular volume and visual acuity, although only borderline significance was demonstrated (P = 0.07). It was concluded that percentage disruption of the [ISel] band is an important predictor of visual acuity among diabetic macular edema patients [41].
B) Our earlier study showed for the first time that disruption of the ELM occurred even before disruption of the ISel band [10]. The ELM is considered to be part of the blood-retinal barrier that can become disrupted by pathologic conditions like diabetic retinopathy, and thus result in fluid accumulation within the macula [42]. Foreshortening of the photoreceptor inner segments might be a secondary consequence of such ELM insult and fragmentation [43].
ISel and ELM band disruption were graded as follows:
• Grade 0: No disruption of ELM and ISel
• Grade 1: ELM disruption, intact ISel
• Grade 2: Both ELM and ISel disrupted
A statistically significant positive correlation was found between logMAR visual acuity and grade of disruption (r=0.85, p<0.0001) [10].
C) Our most recent study demonstrated a simplified, comprehensive and physician friendly approach to grading ISel disruption based on OCT findings. The inner segment-ellipsoid band was studied using horizontal and vertical SD-OCT scans through the fovea. The integrity of this layer was evaluated by two experienced observers, masked to the status of diabetic retinopathy. ISel disruption was graded as follows:
• Grade 0: intact ISel
• Grade 1: focal disruption (localized, subfoveal ISel disruption)
• Grade 2: global disruption (generalized ISel disruption throughout the macular cube)
Above two classifications mentioned by us are physician friendly and easy to recall.
Eyes without retinopathy were found to havea normal ISel. Normal ISel was observed in 7.5% eyes with NPDR (Figure 1). Focal ISel disruption was observed in 62.5% eyes with NPDR and 27.5% eyes with PDR. Global ISel disruption was observed in 25% eyes with NPDR and 72.5% eyes with PDR. Increased severity of retinopathy was associated with increased ISel disruption, graded ‘focal’ to ‘global’ (r = 0.49, p < 0.001) (Figure 2). Furthermore, decreased visual acuity was associated with increased grade of ISel disruption (r = 0.67, p < 0.001), and a marked decrease in visual acuity was found to be associated with global disruption, specifically [44].
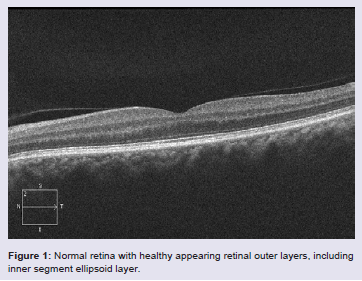
Figure 1: Normal retina with healthy appearing retinal outer layers, including inner segment ellipsoid layer.
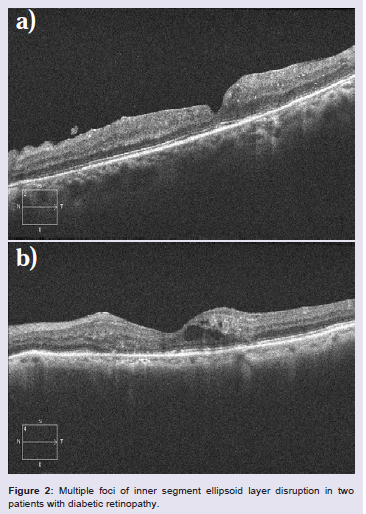
Figure 2: Multiple foci of inner segment ellipsoid layer disruption in two patients with diabetic retinopathy.
The four classification groups were as follows:
CME I – Cysts less than (30%) of macular thickness
CME II – Cysts between 30% and 60% of macular thickness
CME III – Cysts between 60% and 90% of macular thickness
CME IV – Cyst more than 90% of macular thickness.
Each grade was then subdivided according to certain morphologicfeatures using labels ‘A’, ‘B’, ‘C’, and ‘D’:
A – Cysts without any disruption to the ELM or ISel bands
B – Cysts with ELM disruption
C – Cysts with ISeldisruption
D – Cysts with disruption of both ELM and ISel bands
Additionally, the presence of hyper-reflective foci in the outer retinal layers from the ELM to the retinal pigment epithelium within the 1 mm scanned area centered on the fovea was designated with “+” signs [45].
Small hyper-reflective foci can be less than 30 μm in diameter and might not be identified on fundus biomicroscopy, fluorescein angiography, or infrared imaging. They may represent tiny intraretinal protein and/or lipid deposits as they have hyper-reflectivity similar to that of the accumulated spots in an area of hard exudates [46]. The accumulation of hyper-reflective foci in the subretinal spaces indicates a poor prognosis in diabetic macular edema [47]. The presence of hyper-reflective foci in the outer retina is closely associated with ELM and ISel band disruption, and decreased visual acuity in diabetic macular edema [48]. It might also predict photoreceptor damage and a poor prognosis after vitrectomy for DME [49]. Inclusion of hyperreflective foci provided valuable information on the degree of bloodretinal barrier breakdown and its influence on visual acuity.
E) Another classification system was proposed to overcome the limitation of variability in the reflectivity levels of continuous [ISel] bands, seenon SD-OCT. For this, quantification of the status of the transverse length of each segment of the [ISel] band was performed. Classifications were as follows:Intact line– highly reflective and continuous line (physiologic)Faint line – presence of a continuous line with lower reflectivity (less than half of the OCT reflectivity of the RPE)
Disrupted line – absent or discontinuous line
A measurement of the transverse length of each disrupted [ISel] section was also obtained.
SD-OCT reflectivity in the ELM band was similarly analyzed. Relatively homogeneous and continuous ELM bands were described as intact. Absent of discontinuous ELM bands were described as disrupted.
A measurement of the transverse length of each ELM band section was also obtained.
Statistical analysis demonstrated that the total additive transverse length of disrupted [ISel] within the fovea correlated more closely with logMAR visual acuity than did foveal thickness measurements (p = 0.002) [50].
ISel Band Integrity and Pharmacological/Surgical Intervention
Few interventional studies have been conducted to evaluate the relationship between pharmacologic and surgical intervention and ISel band integrity. In one study consisting of eleven eyes with resolved macular edema following pars plana vitrectomy with internal limiting membrane peel for diabetic macular edema, the integrity of the ELM and photoreceptor ISel band was evaluated by SD-OCT. On linear regression analysis, a statistically significant association was found betweenvisual acuity and intact ELM and ISel bands [51].In a retrospective interventional study, 61 eyes of 52 patients with DME who were successfully treated with intravitreal triamcinolone were studied. Based on the restoration of photoreceptor ISel and ELM bands on SD-OCT at final visit, the eyes were divided into three groups:
(1) Group A- completely visible ISel band and ELM
(2) Group B- disruption of ISel band and intact ELM
(3) Group C- disruption or loss of the ISel band and ELM.
It was concluded that integrity of the photoreceptor ISel band correlated well with final best corrected visual acuity (BCVA). Final BCVA of both Group A and Group B was better than that of Group C. They also concluded that shorter lengths of both ISel band and ELM band disruption were both associated with better BCVA. On multivariate analysis, however, it was found that mean disrupted ISel and ELM band length showed greater correlation to final BCVA thanlength of either disrupted ISel band or ELM band taken alone. Another significant conclusion was made that initial visual acuity (prior to treatment) and photoreceptor status can both assist in predicting the post-treatment recovery of the photoreceptor ISel band, and subsequent visual recovery [52].
Another retrospective interventional study was conducted on 61 patients with DME who received intravitreal bevacizumab. Pre- and post-injection assessment of visual acuity, fundus autofluorescence (FAF) and SD-OCT imaging was performed. Foveal FAF was graded n a scale of 1 to 4. Better pre-injection visual acuity and intact photoreceptor ISel band and ELM were associated with better visual acuity after treatment. Significantly increased FAF was seen in cystoid macular edema. FAF was 5.6 times more likely to occur in DME with associated ISel band disruption. It was concluded that correlation between FAF with SD-OCT and visual acuity can help predict restoration of photoreceptor ISel band integrity [53].
Wakabayashi retrospectively reviewed 41 eyes of 41 patients with DME who underwent vitrectomy. Associations between axial length, post-operative BCVA and visibility of photoreceptor ISel band on SD-OCT were studied. Wakabayashi observed that median axial length was longer in those with a visible photoreceptor ISel band at 12 months after surgery, and that longer axial length predictedbetter visual outcomes after vitrectomy in patients with DME [54]. The mechanism of this protective effect was not fully elucidated, but a similar relationship has been established between axial length and DME, as well as diabetic retinopathy itself [55]. This protective effect is presumed to be secondary to an inverse relationship between axial length and ocular blood flow, a parameter attributed to stretchinduced microvascular anatomical changes, such as vessel thinning, that appear to result in diminished pressure against the vascular wall, and a resultant decrease in microvascular leakage and damage to the retinal microstructure [56].
Conclusion
The inner segment ellipsoid band, the second highly reflective outer band seen on OCT, is a well demarcated microstructural layer seen on OCT imaging. Previously, this microstructure was believed to represent the junction between the inner and outer segments ofretinal photoreceptors. Now redefined, the ISel is regarded as a useful hallmark of foveal photoreceptor layer health, and the integrity of which correlates well with final visual acuity and response to treatment in DME.References
- Bjork S, Kapur A, King H, Nair J, Ramachandran A (2003) Global policy: aspects of diabetes in India. Health Policy 66: 61-72.
- King H, Rewers M (1991) Diabetes in adults is now a Third World problem. The WHO Ad Hoc Diabetes Reporting Group. Bull World Health Organ 69: 643-648.
- Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, et al. (2014) Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract 103: 137-149.
- Sharma S, Oliver-Fernandez A, Liu W, Buchholz P, Walt J (2005) The impact of diabetic retinopathy on health-related quality of life. Curr Opin Ophthalmol 16: 155-159.
- Patz A, Schatz H, Berkew JW, Gittelsohn AM, Ticho U (1973) Macular edema--an overlooked complication of diabetic retinopathy. Trans Am Acad Ophthalmol Otolaryngol 77: OP34-42.
- Diabetic Retinopathy study (1981) Report number 7. A modification of the Airline House Classification of diabetic retinopathy. Invest Ophthalmol Vis Sci 21: 210-226.
- Otani T, Kishi S, Maruyama Y (1999) Patterns of diabetic macular edema with optical coherence tomography. Am J Ophthalmol 127: 688-693.
- Gupta V, Gupta A, Dogra MR (2010) Introduction to OCT, Atlas – Optical coherence tomography of macular diseases and glaucoma, 3rd Edition, p. 3-46.
- Goebel W, Kretzchmar-Gross T (2002) Retinal thickness in diabetic retinopathy: a study using optical coherence tomography (OCT). Retina 22: 759-767.
- Jain A, Saxena S, Khanna VK, Shukla RK, Meyer CH (2013) Status of serum VEGF and ICAM-1 and its association with external limiting membrane and inner segment-outer segment junction disruption in type 2 diabetes mellitus. Mol Vis 19: 1760-1768.
- Uji A, Murakami T, Akagi T, Nishijima K, Akagi T, Horii T, et al. (2012) Association between hyperreflective foci in the outer retina, status of photoreceptor layer, and visual acuity in diabetic macular edema. Am J Ophthalmol 153: 710-717.
- Yanyali A, Bozkurt KT, Macin A, Horozoglu F, Nohutcu AF (2011) Quantitative assessment of photoreceptor layer in eyes with resolved edema after pars plana vitrectomy with internal limiting membrane removal for diabetic macular edema. Ophthalmologica 226: 57-63.
- Shin HJ, Lee SH, Chung H, Kim HC (2012) Association between photoreceptor integrity and visual outcome in diabetic macular edema. Graefes Arch Clin Exp Ophthalmol 250: 61-70.
- Chang LK, Koizumi H, Spaide RF (2008) Disruption of the photoreceptor inner segment-outer segment junction in eyes with macular holes. Retina 28: 969-975.
- Spaide RF, Koizumi H, Freund KB (2008) Photoreceptor outer segment abnormalities as a cause of blind spot enlargement in acute zonal occult outer retinopathy-complex diseases. Am J Ophthalmol 146: 111-120.
- Wang NK, Chou CL, Lima LH, Cella W, Tosi J, et al. (2009) Fundus autofluorescence in cone dystrophy. Doc Ophthalmol 119: 141-144.
- Oh J, Smiddy WE, Flynn HW Jr, Gregori G, Lujan B (2010) Photoreceptor inner/outer segment defect imaging by spectral domain OCT and visual prognosis after macular hole surgery. Invest Ophthalmol Vis Sci 51: 1651-1658.
- Inoue M, Morita S, Watanabe Y, Kaneko T, Yamane S, et al. (2010) Inner segment/outer segment junction assessed by spectral-domain optical coherence tomography in patients with idiopathic epiretinal membrane. Am J Ophthalmol 150: 834-839.
- Hood DC, Lazow MA, Locke KG, Greenstein VC, Birch DG (2011) The transition zone between healthy and diseased retina in patients with retinitis pigmentosa. Invest Ophthalmol Vis Sci 52: 101-108.
- Kitaguchi Y, Kusaka S, Yamaguchi T, Mihashi T, Fujikado T (2011) Detection of photoreceptor disruption by adaptive optics fundus imaging and Fourier-domain optical coherence tomography in eyes with occult macular dystrophy. Clin Ophthalmol 5: 345-351.
- Drexler W, Sattmann H, Hermann B, Ko TH, Stur M, et al. (2003) Enhanced visualization of macular pathology with the use of ultrahigh-resolution optical coherence tomography. Arch Ophthalmol 121: 695-706.
- Ko TH, Fujimoto JG, Duker JS, Paunescu LA, Drexler W, et al. (2004) Comparison of ultrahigh- and standard- resolution optical coherence tomography for imaging macular hole pathology and repair. Ophthalmology 111: 2033-2043.
- Srinivasan VJ, Ko TH, Wojtkowski M, Carvalho M, Clermont A, et al. (2006) Noninvasive volumetric imaging and morphometry of the rodent retina with high-speed, ultrahigh-resolution optical coherence tomography. Invest Ophthalmol Vis Sci 47: 5522-5528.
- Srinivasan VJ, Monson BK, Wojtkowski M, Bilonick RA, Gorczynska I, et al. (2008) Characterization of outer retinal morphology with high-speed, ultrahigh-resolution optical coherence tomography. Invest Ophthalmol Vis Sci 49: 1571-1579.
- Zawadzki RJ, Jones SM, Olivier SS, Zhao M, Bower BA, et al. (2005) Adaptive-optics optical coherence tomography for high- resolution and high-speed 3D retinal in vivo imaging. Opt Express 13: 8532-8546.
- Puche N, Querques G, Benhamou N, Tick S, Mimoun G, et al. (2010) High-resolution spectral domain optical coherence tomography features in adult onset foveomacular vitelliform dystrophy. Br J Ophthalmol 94: 1190-1196.
- Spaide RF, Curcio CA (2011) Anatomical correlates to the bands seen in the outer retina by optical coherence tomography: literature review and model. Retina 31: 1609-1619.
- Drexler W, Sattmann H, Hermann B, Ko TH, Stur M, et al. (2003) Enhanced visualization of macular pathology with the use of ultrahigh-resolution optical coherence tomography Arch Ophthalmol 121: 695-706.
- Anger EM, Unterhuber A, Hermann B, Sattmann H, Schubert C, et al. (2004) Ultrahigh- resolution optical coherence tomography of the monkey fovea: Identification of retinal sublayers by correlation with semithin histology sections. Exp Eye Res 78: 1117-1125.
- Spaide RF (2012) Questioning optical coherence tomography. Ophthalmology 119: 2203-2204.
- Krebs W, Krebs I (1991) Primate retina and choroid: Atlas of fine structure in man and monkey. New York, NY: Springer Verlag.
- Hogan JA, Alvarado MJ, Weddell JE (1971) Histology of the human eye. An atlas and textbook. WB Saunders. Philadelphia, PA, 328-363.
- Fernandez EJ, Hermann B, Povazay B, Unterhuber A, Sattmann H, et al. (2008) Ultrahigh-resolution optical coherence tomography and pancorrection for cellular imaging of the living human retina. Opt Exp 16: 11083-11094.
- Lu RW, Curcio CA, Zhang Y, Zhang QX, Pittler SJ, et al. (2012) Investigation of the hyper-reflective inner/outer segment band in optical coherence tomography of living frog retina. J Biomed Opt 17: 060504.
- Kim BY, Smith SD, Kaiser PK (2006) Optical coherence tomographic patterns of diabetic macular edema. Am J Ophthalmol 142: 405-412.
- Martidis A, Duker JS, Greenberg PB, Rogers AH, Puliafito CA, et al. (2002) Intravitreal triamcinolone for refractory diabetic macular edema. Ophthalmology 109: 920-927.
- Yamamoto S, Yamamoto T, Hayashi M, Takeuchi S (2001) Morphological and functional analyses of diabetic macular edema by optical coherence tomography and multifocal electroretino- grams. Graefes Arch Clin Exp Ophthalmol 239: 96-101.
- Strøm C, Sander B, Larsen N, Larsen M, Lund-Andersen H (2002) Diabetic macular edema assessed with optical coherence tomography and stereo fundus photography. Invest Ophthalmol Vis Sci 43: 241-245.
- Nunes S, Pereira I, Santos A, Bernardes R, Cunha-Vaz J (2010) Central retinal thickness measured with HD-OCT shows a weak correlation with visual acuity in eyes with CSME. Br J Ophthalmol 94: 1201-1204.
Diabetic Retinopathy Clinical Research Network, Browning DJ, Glassman AR, Aiello LP, Beck RW, et al. (2007) Relationship between optical coherence tomography-measured central retinal thickness and visual acuity in diabetic macular edema. Ophthalmology 114: 525-536.- Maheshwary AS, Oster SF, Yuson RM, Cheng L, Mojana F, et al. (2010) The association between percent disruption of the photoreceptor inner segment-outer segment junction and visual acuity in diabetic macular edema. Am J Ophthalmol 150: 63-67.
- Omri S, Omri B, Savoldelli M, Jonet L, Thillaye-Goldenberg B, et al. (2010) The outer limiting membrane (OLM) revisited: clinical implications. Clin Ophthalmol 4: 183-195.
- Mehalow AK, Kameya S, Smith RS, Hawes NL, Denegre JM, et al. (2003) CRB1 is essential for external limiting membrane integrity and photoreceptor morphogenesis in the mammalian retina. Hum Mol Genet 12: 2179-2189.
- Sharma SR, Saxena S, Mishra N, Akduman L, Meyer CH (2014) The association of grades of photoreceptor inner segment-ellipsoid band disruption with severity of retinopathy in type 2 diabetes mellitus. J Case Rep Stud 2: 205.
- Helmy YM, Atta Allah HRA (2013) Optical coherence tomography classification of diabetic cystoid macular edema. Clin Ophthalmol 7: 1731-1737.
- Bolz M, Schmidt-Erfurth U, Deak G, Mylonas G, Kriechbaum K, (2009) Optical coherence tomographic hyper reflective foci: a morphologic sign of lipid extravasation in diabetic macular edema. Ophthalmol 116: 914-920.
- Ota M, Nishijima K, Sakamoto A, Murakami T, Takayama K, et al. (2010) Optical coherence tomographic evaluation of foveal hard exudates in patients with diabetic maculopathy accompanying macular detachment. Ophthalmol 117: 1996-2002.
- Uji A, Murakami T, Nishijima K, Akagi T, Horii T, et al. (2012) Association between hyperreflective foci in the outer retina, status of photoreceptor layer, and visual acuity in diabetic macular edema. Am J Ophthalmol 153: 710-717.
- Nishijima K, Murakami T, Hirashima T, Uji A, Akagi T, et al. (2014) Hyperreflective foci in outer retina predictive of photoreceptor damage and poor vision after vitrectomy for diabetic macular edema. Retina 34: 732-740.
- Murakami T, Nishijima K, Akagi T, Uji A, Horii T, et al. (2012) Optical coherence tomographic reflectivity of photoreceptors beneath cystoid spaces in diabetic macular edema. Invest Ophthalmol Vis Sci 53: 1506-1511.
- Yanyali A, Bozkurt KT, Macin A, Horozoglu F, Nohutcu AF (2011) Quantitative assessment of photoreceptor layer in eyes with resolved edema after pars plana vitrectomy with internal limiting membrane removal for diabetic macular edema. Ophthalmologica 226: 57-63.
- Shin HJ, Lee SH, Chung H, Kim HC (2012) Association between photoreceptor integrity and visual outcome in diabetic macular edema. Graefes Arch Clin Exp Ophthalmol 250: 61-70.
- Chung H, Park B, Shin HJ, Kim HC (2012) Correlation of fundus autofluorescence with spectral-domain optical coherence tomography and vision in diabetic macular edema. Ophthalmology 119: 1056-1065.
- Wakabayashi Y, Kimura K, Muramatsu D, Usui Y, Umazume K, et al. (2013) Axial length as a factor associated with visual outcome after vitrectomy for diabetic macular edema. Invest Ophthalmol Vis Sci 54: 6834-6840.
- Man RE, Sasongko MB, Sanmugasundram S, Nicolaou T, Jing X, et al. (2012) Longer axial length is protective of diabetic retinopathy and macular edema. Ophthalmology 119: 1754-1759.
- Quigely M, Cohen S (1999) A new pressure attenuation index to evaluate retinal circulation. A link to protective factors in diabetic retinopathy. Arch Ophthalmol 117: 84-89.