
Journal of Urology & Nephrology
Download PDF
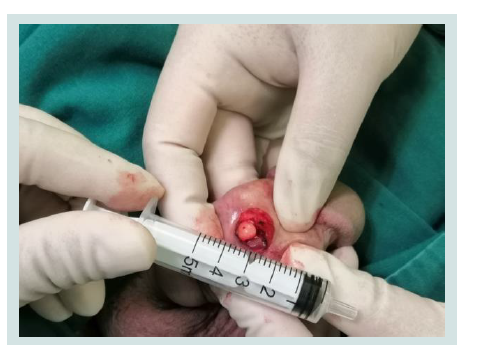 Figure 1: The mass locating in the dorsal of the penis.
Figure 1: The mass locating in the dorsal of the penis.
 Figure 2: The gross appearance of the mass.
Figure 2: The gross appearance of the mass.
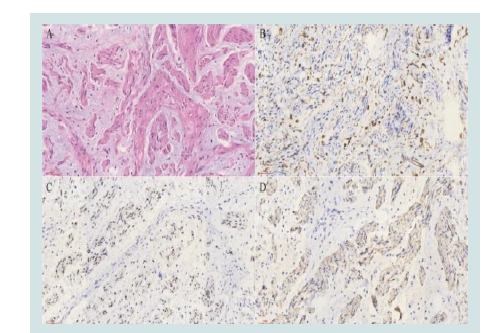 Figure 3: Immunohistochemistry study of the penile myxoid neurofibroma. Bars above, 60μm. A, HE; B, CD34; C, SOX10; D, S100.
Figure 3: Immunohistochemistry study of the penile myxoid neurofibroma. Bars above, 60μm. A, HE; B, CD34; C, SOX10; D, S100.
Case Report
A Rare Case of Myxoid Neurofibroma of the Penis and the Literature Review
Cheng S1, Yang J2*, Zhang Y1, Xu An1, Dong Li1 and Yang G1
1Department of Urology, Tongren Hospital, Shanghai Jiao Tong University School of Medicine, China
2Department of Pathology, Tongren Hospital, Shanghai Jiao Tong University School of Medicine, China
*Address for Correspondence: Yang G, Department of Urology, Tongren Hospital, Shanghai Jiao Tong University School of Medicine, Email: Yangg1103@126.com
Submission: 11 January, 2021;
Accepted: 15 February, 2021;
Published: 17 February, 2021
Copyright: © 2021 Cheng S, et al. This is an open access article
distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Abstract
Neurofibroma (NF) is an autosomal dominant genetic disease, which can be divided into two subtypes: NF-1 and NF-2. In the genitourinary system, NF-1 was usually found in the bladder, it in the penis is extremely
rare, to improve the diagnosis and treatment of the disease, in the present case, myxoid NF-1 occurring in the penis was reported.
Introduction
Neurofibroma (NF) is an autosomal dominant genetic disease,
which can be divided into two subtypes: NF-1 often occurs in
peripheral nerves and is mainly related to mutations of nf-1 gene;
NF-2 is rare, and it usually occurs in the central nervous system.
NF-1 in the genitourinary system usually occurs in the bladder [1],
however, NF-1 with myxoid degeneration occurring in the penis has
not been reported. To improve the diagnosis and treatment of the
disease, a 33-year-old patient with myxoid NF-1 of the penis has been
reported in this case.
Case Presentation
A patient, a 33-year-old male, came to our center with the
compliant for a penile mass for 1 month. He complained that a mass
in penile was found accidentally, without sexual pain and abnormal
erectile function. He had no trauma history in perineum. Since being
noted, the mass has been progressively enlarged within the month.
After admission, Physical examination revealed a healthy looking, not
pale. No obvious abnormality was found in abdomen. Genitourinary
examination showed that the patient had a mass in the dorsal center
of the penis about 1.5 cm away from the coronal sulcus, with a size
of about 0.8 × 0.5 cm and no haphalgesia, no adhesion to the skin
and spongy body, with good mobility. The foreskin is long, without
edema. No swelling nodule was found in bilateral groin.
After admission, the patient has carried on the related preoperative
examination. After excluding surgery contraindications, he was
conducted 1% lidocaine local infiltration anesthesia for penile dorsal
tumor resection, the mass in the dorsal center of the penis about 1.5 cm
away from the coronal sulcus. While the mass was found closing to
penile left dorsal nerve bundle (Figure 1), there is no adhesion and
the surface is smooth (Figure 2). The surgical resection was carried
out in a smooth manner, and the incision healed well one week after
the operation. Postoperative pathological studies showed S100, CD34
and SOX10 were all positive deducing a diagnosis of myxoid NF-1
(Figure 3). The patients were followed up for 2 years after operation,
and there was no recurrence, abnormal sexual function.
Discussion
NF is a common autosomal dominant genetic disease with a prevalence of about 1/3000 ~ 1/3500 [2]. NF can be classified into
two subtypes according to the characteristics of skin lesions and
neuropathy [3]: NF-1 often occurs in peripheral nerves and is mainly
related to mutations of nf-1 gene, accounting for 90% of the total
incidence. NF-1 is mostly superficial neurofibroma, the most common
being plexiform neurofibroma. Plexus neurofibroma is considered
to be a benign lesion histologically. The common components of
neurofibroma are neuroaxons, Schwann cells, fibroblasts, mast cells,
macrophages, peripheral nerve cells, and extracellular matrix, such as
collagen. NF-1 is caused by the heterozygous mutation of nf-1 gene.
The neurcellulose encoded by nf-1 gene has the function of expressing
or down-regulating neurofibrin. When nf-1 is mutated, it will lead
to the loss of neurofibrin expression, thus leading to NF-1 lesions.
NF-2 is a subtype in which the central nervous system is frequently
involved. The most common symptom is a sudden hearing loss, often
caused by unilateral or bilateral vestibular schwannomas.
Pathologically, NF is a benign tumor of the nerve sheath, usually
with soft or rubbery
Pathologically, NF is a benign tumor of the nerve sheath, usually
with soft or rubbery in texture [4]. Histopathological manifestations of NF include classical, myxiod, cellular, transparent, plexiform,
epithelioid, diffuse, Parkini, pigmentation, and granulosa cell types.
NF associated with mucin deposition including typical, mucinous,
cellular, and plexiform nerve fibers [5]. NF-1 could occur in any part of the body, can continue to grow throughout life, and can be life-threatening due to compression of
important structures, malignant transformation into neurosarcoma,
or peripheral schwannomas. The lesions of NF-1 include milk and coffee spots on the skin, axillary or inguinal freckles, Lisch nodules
on the iris, dysplasia of long bones and mental retardation. The
lesions are mainly manifested as multiple nervous system tumors,
skin pigmentation spots, vascular system and other visceral lesions.
NF located in the penile body is reported in 1 case reported with the
subtype of plexiform [3]. Although the myxoid NF often occurs in
the face, shoulders and upper limbs, while myxoid NF in the penis
has not been reported.
The differential diagnosis of NF-1 is commonly including
tuberous sclerosis, McCune-abright syndrome and Proteus syndrome.
The Myxoid differential diagnosis of NF should be distinguished
from Spindle cell lipoma, Myxoma, Myxoid Liposarcoma, Myxoid
Dermatofibromas Protuberans, and low-grade fibromyxoid
Sarcoma. Although the occurrence of NF-1 in the penis is extremely
rare, the possibility of the diagnosis should be considered to avoid
misdiagnosis.
As a common benign lesion, the diagnosis of NF depends on the
detection of pathological molecular markers, which could include
S100 positive Schwann cells, CD34 and SOX10, and the 3 molecular
markers in our case were all positive. The treatment of NF is mainly
surgical resection, and the prognosis is good. The patient was regularly
followed up for 2 years without tumor recurrence. There were several
reports showed that the NFs in penis were benign lesions which have
good consequence.
Conclusion
NF is an autosomal dominant hereditary disease. The Myxoid NF
can also occur in the penis. Thus, when a lesion occurred in the site
for diagnosis, Myxoid NF should be considered
References
Citation
ChengS, Yang J, Zhang Y, Xu An, Dong Li, Yang G. A Rare Case of Myxoid Neurofibroma of the Penis and the Literature Review. J Urol Nephrol. 2021;8(1): 2.