
Journal of Veterinary Science & Medicine
Download PDF
 Figure 1:A dog with coat discoloration due to hypocobalaminemia. Left:
After 6 months of diarrhoea (before treatment). Right: 6 months after start
of treatment.
Figure 1:A dog with coat discoloration due to hypocobalaminemia. Left:
After 6 months of diarrhoea (before treatment). Right: 6 months after start
of treatment.
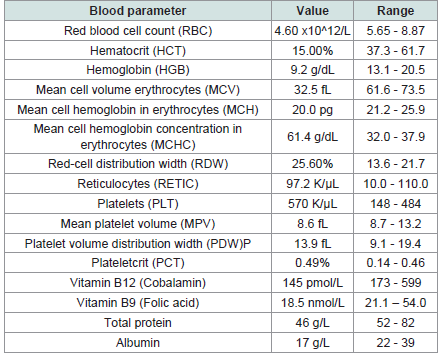 Table 1:Relevant blood analysis values after 6 months of symptoms
Table 1:Relevant blood analysis values after 6 months of symptoms
Case Report
Case Report: Hypocobalaminemia and Coat Discoloration in A Dog
Mik M De* and Corbee RJ
Faculty of Veterinary Medicine, Utrecht University, Utrecht, The Netherlands
*Address for correspondence: Mik M De, Faculty of Veterinary Medicine, Utrecht University, Utrecht,
The Netherlands, E-mail Id:m.demik@uu.nl
Submission:01 March, 2024
Accepted:10 April, 2024
Published:15 April, 2024
Copyright:© 2024 De MM, et al. This is an open access article
distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Keywords: Canine; Cobalamin; Vitamin B12 Deficiency; Coat
Discoloration; Hair Depigmentation; Chronic Diarrhoea
Abstract
Hypocobalaminemia is a common complication in case of
chronic diarrhoea in dogs. Reduced cobalamin (vitamin B12) causes
diarrhoea, creating a viscous circle.
A 10-year-old male intact Frisian pointing dog (18.9 kg; BCS 4/9)
was presented to the primary care veterinarian diarrhoea. After
6 months of chronic diarrhoea with symptomatic treatments, lab
analysis showed a reduction of cobalamin (145 pmol/L; reference 173-
599) and folic acid (18.5 nmol/L; reference 21.1-54.0). Consistent with
hypocobalaminemia, a nonregenerative anaemia was found.
Treatment consisted of weekly injections of 1 mg vitamin B12 (for 6
weeks) and the months of supplementation per os. Six months after the
treatment, the discoloration was resolved.
The mechanism of coat discoloration due to hypocobalaminemia
is unclear, but multiple cases in humans are known. Vitamin B12
is supposed to influence melanin to impact the coat colour. To the
authors’ knowledge, this is the first case in dogs of hypocobalaminemia
resulting in coat discoloration.
Introduction
Cobalamin, vitamin B12, is an essential water-soluble vitamin. It
functions as a cofactor for both homocysteine methyl transferase and
methylmalonyl-CoA mutase. Primary, the cytosolic homocysteine
methyltransferase is facilitating the conversion of homocysteine to
methionine, which also requires folic acid as cofactor. Following this
pathway, pyrimidines and purines can be produced for DNA and RNA
synthesis. Secondary, the mitochondrial methylmalonyl-CoA mutase
is involved in the enzymatic degradation of fatty acids. Consequently,
cobalamin is essential for myelin synthesis, haematopoiesis, and
DNA synthesis [1-4].
The gastrointestinal absorption of vitamin B12 is complex,
consequently a hypocobalaminemia is comprehensible. During
digestion, three indispensable steps are compulsory. Firstly, in
the stomach, cobalamin is separated from dietary protein by
gastric pepsin and bound to protect haptocorrin from bacterial
fermentation. Secondly in the small intestine, cobalamin is separated
from haptocorrin by pancreatic proteases and forms a complex with
intrinsic factor (IF). In dogs, IF is primarily produced in the pancreas.
Thirdly, the complex of IF and cobalamin absorbed via active
transport in the distal ileum. Plants contain practically no cobalamin
since their enzymes do not depend on this vitamin; all vitamin
B12 in animal feed originates either from animal products or from
bacterial fermentation. Nonetheless, the location of absorptionoccurs
proximal of the site of bacterial fermentation in dogs. Consequently,
all cobalamin produced by bacterial fermentation is excreted in the
faeces. Due to the complexity of the absorption and the essential
role of the exocrine pancreas and the limited absorption area,
hypocobalaminemia can be initiated by gastrointestinal disease.
Particularly in case of exocrine pancreatic insufficiency and severe
chronic ileal disease can lead to hypocobalaminemia [2-4].
The clinical pathologic symptoms for dogs with low vitamin
B12 typically concentrate in two areas: blood cell abnormalities
and neurological signs. Megaloblastic nonregenerative anaemia,
hypersegmented neutrophils,and neutropenia, are signs
ofearlyhypocobalaminemia in dogs. Secondary, diarrhoea, vomiting,
anorexia and lethargy can be observed. Since cobalamin (as well as
folic acid) deficiency can result in signs of vomiting and diarrhoea,
a vicious circle can occur. Hence, veterinarians should be alert to the
possibility of vitamin B12 deficiency in case of chronic diarrhoea,
both primary and secondary [4].
The current case report describescoat discoloration in a dog with
hypocobalaminemia. The aim of this paper is to present the potential
pathophysiological correlation between vitamin B12 and coat colour
in dogs.
Materials and Methods
A 10-year-old male intact Frisian pointing dog (18.9 kg; BCS
4/9) was presented to the primary care veterinarian with acute small
bowel diarrhoea. Other signs included: vomiting, reduced appetite
and lethargy. Neurological abnormalities or signs of malabsorption
were not present.
Results
First treatment by the primary care veterinarian was symptomatic
with maropitant. The original food (i.e.,HillsTM prescription dietj/d
canine) was not changed. Six months after first presentation, the
gastrointestinal problems worsened: daily vomiting and diarrhoea.
Both vomiting and diarrhoea was without blood incorporation.
Additionally, a clear discolouration of the coat appeared see (Figure
1). The treatment consisted of omeprazole/maropitant and food
change to HillsTM prescription dieti/d canine chicken. Secondary
to this treatment, the dog was medicated with carprofen continuously
for osteoarthritis.
Two weeks later the symptoms did persist, so extensive blood
analysis was performed [Table 1], apart from continuation of
the symptomatic treatment. Metronidazole was added to the treatment
plan, even though the giardia analysis was negative. Additionally, the
dog was treated orally with milbemycin/preziquantel every quarter
and was negative for faecal parasites.
The lab analysis showed that both cobalamin (145 pmol/L;
reference 173-599) and folic acid (18.5 nmol/L; reference 21.1-
54.0) were reduced. Consistent with hypocobalaminemia, a
nonregenerative anaemia was found.
After six months of having diarrhoea with symptomatic
treatment, the treatment against hypocobalaminemia was started: the
dog was treated weekly with 1 mg vitamin B12 injections (6 weeks)
and supplementation per os (3 months). Three weeks after starting
the vitamin B12 injections, the diarrhoea was cured. Subsequently,
the coat discoloration was resolved 6 months later see [Figure 1].
Discussion
The primary cause of diarrhoea remains indefinit. Adverse effects
of NSAIDs have been reported in multiple and commonly included
vomiting, diarrhoea, and anorexia [5] which wasqual to the observed
signs. However, the administration of carprofen has not been changed
while the clinical signs weren solved. However, carprofen combined
with omeprazole has shown to induce faecal dysbiosis and increase
intestinal inflammatory markers in otherwise healthy dogs [6].This
coadministration of both medicines could have contributed to the
continuation of the diarrhoea and thereby adding to the demised
absorption of vitamin B12. Still, omeprazole has only been given 6
months after the first representation. Subsequently, these treatments
cannot be diagnosed as the primary cause of the diarrhoea.
Dogs with vitamin B12 deficiency show a variety of signs such
as anorexia, lethargy, diarrhoea, nonregenerative anaemia, and
neurological signs [4]. All clinical signs, except for the neurological
abnormalities, were present. With respect to blood parameters, the
serum level of cobalamin is no sufficient evidence for a conclusive
diagnosis. The intracellular shortage of vitamin B12 results in a lower
enzyme activity rather than the level in the serum. To correlate serum
values to intracellular levels, a raise in methylmalonic acid or an
increased homocysteine level in serum can be used for diagnosis. It
has to be considered that reduced homocysteine level can be analysed
in case of a folate deficiency [4,7]. Since both folic acid and cobalamin
showed decreased serum values, a primary hypocobalaminemia
based on blood values alone was inconclusive. Secondary analysis of
methylmalonic acid and homocysteine could be used to confirm the
diagnosis. Additionally, the additional serum measurements could
contribute to a differentiation between a deficiency of cobalamin
and folic acid; methylmalonic acid is not influenced by a folic acid
deficiency. Retrospectively, the vitamin B12 injections proved
successful without supplementation of folic acid, proving the
hypocobalaminemia as true by therapeutic diagnostics.
With respect to coat discoloration, no cases have been
reported in dogs to the author’s knowledge.In humans, reversible
hyperpigmentation of the skin and depigmentation of the hair
has been reported in some cases of vitamin B12 deficiency. In case
reported by [8], vitamin B12 substitution resulted in normalizing
serum B12 levels and a decrease of skin hyperpigmentation, but
hair depigmentation remained. Histopathological findings showed
increased levels of melanin in the basal layer of the epidermis in these
patients. However, the exact underlying mechanism remain unknown
in humans as well, especially due to the apparent contradictory
depigmentation of the hair versus the hyperpigmentation of the skin
persists to be ambiguous.
Deposited melanin is responsible for hair and skin pigmentation.
Melanin is produced by melanocytes, whereafter melanin-containing
granules (melanosomes) are exported to neighbouring keratinocytes.
The skin pigmentation is the result of melanin in these keratinocytes.
[9,10]. In hair follicles, the keratocytes containing melanin form
the pigmented hair shaft [11]. A single melanocyte can serve 40
keratinocytes. The density of melanocytes is similar in humans for
all skin types, but the amount of melanin and the type of melanin
determines the colouration [10,12].
Two main types of melanin can be found in skin and hair:
pheomelanin (red/yellow colour) and eumelanin (brown/black
colour). The ratio of both melanin types is determined by three
factors: (1) the tyrosinase activity, (2) the concentration of cysteine as
a constituent of pheomelanin, and (3) the concentration of tyrosine
as a component of eumelanin.While tyrosine/cysteine influence the
formation of both its end products, an increased tyrosinase activity
turns up the level of eumelanin [10,12].
Lower levels of B12 have been shown to cause premature
greying of hair in humans, once again without known mechanism.
[13]. It has been hypothesized that vitamin B12 deficiency decreases
the level of glutathione. Glutathione is an essential non-enzymatic
antioxidant in mammalian cells which consists of three amino acids:
cysteine, glycine, glutamate [14]. Pheomelanin generation utilizes the
cysteine from glutathione. This reduction of glutathione stores makes
melanocytes more susceptible to oxidative stress and might lower the
total production of eumelanin and pheomelanin. On the other hand,
melanin is also a potent antioxidant scavenging free radicals [10].
With a potential lower level of glutathione and casual oxidative stress,
melanin could serve as antioxidant.
Conclusion
In conclusion, even though the mechanism of coat discoloration
in correlation to hypocobalaminemia remains unclear, multiple
cases in humans have presented the impact of vitamin B12 on hair
discoloration. Vitamin B12 is supposed to influence melanin to impact
the coat colour. To the authors’ knowledge, the coat discoloration
because of hypocobalaminemia has not yet been described in dogs.
References
Citation
De MM, Corbee RJ. Case Report: Hypocobalaminemia and Coat Discoloration in A Dog. J Veter Sci Med. 2024;12(1): 1