
Journal of Neurology and Psychology
Download PDF
Case Report
*Address for Correspondence: Graham Ewing, Mimex Montague Healthcare Limited, Mulberry House, 6 Vine Farm Close, Cotgrave, Nottingham NG12 3TU, UK, Tel: +44-115-9899618; E-mail: graham.ewing@mmhcl.co.uk
Citation: Ewing G. What is the function of the Brain? What does it do and how does it do it? It functions as a Neuroregulator, which continuously regulates the Autonomic Nervous System and Physiological Systems, and enables us to Recognise that Sleep Exhibits the Characteristics of a Neurally Regulated Physiological System. J Neurol Psychol. 2016; 4(2): 9.
Copyright © 2016 Ewing G. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Neurology and Psychology | ISSN: 2332-3469 | Volume: 4, Issue: 2
Submission: 17 September, 2016 | Accepted: 17 October, 2016 | Published: 22 October, 2016
 Physiological Systems
Physiological Systems
 It is reasonable to conclude therefore that sleep dysfunction contributes to pathological onset, primarily in the visceral organs, and hence must alter or influence autonomic stability; and that such alterations must have biochemical origins e.g. due to variations of (i) the levels of proteins and/or other biologically significant moieties such as fatty acids, nucleosides, minerals and vitamins; (ii) theprevailing reaction conditions which influence the rate and completeness of such genetic and phenotypic reactions and pathological onset/ outcomes e.g. temperature, acidity, levels of minerals; (iii) the levels of thyroid, pituitary or adrenal hormones; and/or (iv) the precise way which stress acts upon the body to produce a spectrum of pathological correlates/metabolites [28].
It is reasonable to conclude therefore that sleep dysfunction contributes to pathological onset, primarily in the visceral organs, and hence must alter or influence autonomic stability; and that such alterations must have biochemical origins e.g. due to variations of (i) the levels of proteins and/or other biologically significant moieties such as fatty acids, nucleosides, minerals and vitamins; (ii) theprevailing reaction conditions which influence the rate and completeness of such genetic and phenotypic reactions and pathological onset/ outcomes e.g. temperature, acidity, levels of minerals; (iii) the levels of thyroid, pituitary or adrenal hormones; and/or (iv) the precise way which stress acts upon the body to produce a spectrum of pathological correlates/metabolites [28].


 Initial research has illustrated how SVS is able to determine the complex pathological correlates which are present in patients with diabetes, cardiovascular disease, depression, Alzheimer´s disease, Raynaud´s phenomenon, etc [31-35]. The reported results are consistent with prevailing observations which indicates that the technique performs at a high level of accuracy, perhaps more accurately than contemporary diagnostic tests [16]. It is able to determine pathological onset at differing levels of physiological significance e.g. at the level of physiological systems, organs, cellular biology and molecular biology (see Figures 1-3). Moreover this data can be used to calculate the precise parameters of a course of SLT.
Initial research has illustrated how SVS is able to determine the complex pathological correlates which are present in patients with diabetes, cardiovascular disease, depression, Alzheimer´s disease, Raynaud´s phenomenon, etc [31-35]. The reported results are consistent with prevailing observations which indicates that the technique performs at a high level of accuracy, perhaps more accurately than contemporary diagnostic tests [16]. It is able to determine pathological onset at differing levels of physiological significance e.g. at the level of physiological systems, organs, cellular biology and molecular biology (see Figures 1-3). Moreover this data can be used to calculate the precise parameters of a course of SLT.
What is the function of the Brain? What does it do and how does it do it? It functions as a Neuroregulator, which continuously regulates the Autonomic Nervous System and Physiological Systems, and enables us to Recognise that Sleep Exhibits the Characteristics of a Neurally Regulated Physiological System
Graham Ewing*
- Mimex Montague Healthcare Limited, Mulberry House, Nottingham, UK.
*Address for Correspondence: Graham Ewing, Mimex Montague Healthcare Limited, Mulberry House, 6 Vine Farm Close, Cotgrave, Nottingham NG12 3TU, UK, Tel: +44-115-9899618; E-mail: graham.ewing@mmhcl.co.uk
Citation: Ewing G. What is the function of the Brain? What does it do and how does it do it? It functions as a Neuroregulator, which continuously regulates the Autonomic Nervous System and Physiological Systems, and enables us to Recognise that Sleep Exhibits the Characteristics of a Neurally Regulated Physiological System. J Neurol Psychol. 2016; 4(2): 9.
Copyright © 2016 Ewing G. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Neurology and Psychology | ISSN: 2332-3469 | Volume: 4, Issue: 2
Submission: 17 September, 2016 | Accepted: 17 October, 2016 | Published: 22 October, 2016
Abstract
The aim of this article is to provoke further discussion of the mechanisms which the brain uses to regulate the body´s function, in particular the autonomic nervous system. It focuses upon an understanding of the structural relationship between the brain, organ networks (more commonly referred to as physiological systems), organs and cellular and molecular biology, brain and illustrates (i) that sleep exhibits the characteristics of a physiological system; (ii) that the brain uses colour and frequency to regulate the body´s complex function; but also (iii) that brain function, including the processes involved in the fixation of memories, is influenced by the level of pathological onset arising from past experiences and/or stress.Such understanding, incorporated into a mathematical model of the autonomic nervous system (developed by I.G. Grakov), has led to the development of Strannik software: Strannik Virtual Scanning & Strannik Light Therapy, and enables us to demonstrate that ‘optimisation of sleep’ is the purpose of a physiologically significant system or network of organs, which is regulated by the brain; that sleep performs a physiologically significant biological function, in particular that during sleep the brain produces hormones which are essential re the processes of recovery, regeneration and regulation; and that emergent pathologies in the various organs in this system, often due to the effect of the many and various stressors in our hyper indulgent and/ or sedentary lives, influences quality and quantity of sleep.
Reported Case Studies illustrate the effectiveness of Strannik Virtual Scanning and Strannik Light Therapy to determine and treat the fundamental pathological origins and/or processes which contribute to, and/or are responsible for, sleep dysfunction.
In conclusion, the article illustrates what the brain does - it is a neural regulator of the autonomic nervous system and physiological systems; and how it does it - it uses frequency and light to regulate the body´s complex biological function.
Keywords
Strannik; Strannik virtual scanning; Strannik light therapy; Human brain project; Autonomic nervous system; Physiological systems; Organ networks; SleepAbbreviations
SVS: Strannik Virtual Scanning; SLT: Strannik Light Therapy; ANS: Autonomic Nervous System; HBP: Human Brain Project; CNS: Central Nervous SystemIntroduction
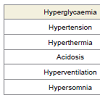
The existence of the Human Brain Project illustrates a recognition, or an acceptance, by the medico-scientific research communities that the brain receives and processes sensory input which influences the stable function of the autonomic nervous system and associated structures; that cognitive properties are influenced by pathological onset; and also that the brain functions at different levels of physiological significance [ Note 1 and 2]. The issue therefore is no longer whether such mechanism(s) exist but instead what are the precise mechanisms involved and how can they be adapted with diagnostic and therapeutic effect, however there is an inconsistency by medical research to such phenomena. On the one hand there is recognition that there are physiological systems - network of organ networks - which are denoted through the use of appendices hyper and hypo function, and recognition that such systems form the fundamental basis of modern medicine, in particular, the doctor´ s examination (e.g. see Table 1). On the other hand the current biomedical paradigm is based upon the measurement of biologically significant markers (biomarkers) and the use of pharmacologically active substances (drugs) - which act upon single biochemical processes - to alter the body´s function and artificially enhance the longevity and quality of sleep however this excludes a comprehensive understanding of:- The nature and significance of sleep;
- The influence which drugs have upon the quality of sleep;
- The function which sleep has upon the body´s overall function; and
- Recognition that sleep dysfunction has complex multisystemic, polygenomic, and complex phenotypic (lifestyle/environmental) origins.
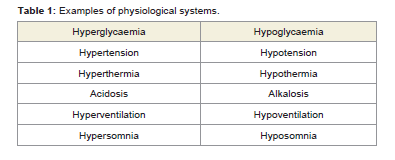
Table 1: Examples of physiological systems.
The alternative way of describing these physiological systems, which varies slightly from the published and accepted description of physiological systems, is of organ systems which have physiological significance - each regulating physiologically important parameters e.g. body temperature, oxygen levels/breathing, heart rate, blood pressure, etc. These organ systems have physiological significance (hence the term ‘physiological or functional systems’) [Note 3 ] (see Table 1). They involve the coherent function of the various organ networks, often referred to as ‘a network of organ networks’ however this raises fundamental issues, in particular:
(i) How are these systems regulated? Biochemistry alone appears to be unable to explain the coherent function of these organ networks, and
(ii) If there are regulated systems what is the significance of the various biomedical and biophysical indices which we use to measure health? Are they the cause or the consequence of the failure of this regulatory mechanism?
(iii) What is the nature of the mechanism by which the body´s function is altered by stress and by biological input?
Moreover, is it conceivable that the physiological systems are the physiological manifestations (genotype and phenotype) and correlates of the basic behavioural traits which preoccupy the human throughout his/her life i.e. our psychosomatic and somatic behaviours appears to be focused upon specific functional or executive outcomes: seeking sustenance (digestion, blood glucose, blood pressure, blood cell content, blood volume); sustaining optimum pO2 at different altitudes (breathing); shelter, comfort and warmth (body temperature); maintaining the existence of the species (sexual function); elimination or excretion of body wastes; regulation of pH, posture and osmotic pressure (salt); and sleep.
In previous articles the author has illustrated that biochemistry alone is unable to explain the body´s complex function [Note 4 ] e.g.
- If measuring the levels of a protein biomarker - how much of the protein is coiled and reactive? There must be a neural mechanism which regulates the body´s pH and hence the coiled/ uncoiled reactive/unreactive nature of protein functions [3].
- Stress is manifest as a spectrum of pathological correlates influencing the function of the brain and the normal levels of homeostasis associated with visceral function.
- Sports physiology involves an understanding that the brain continuously monitors and micro-manages the body´s complex multi-systemic function and stability [4,5].
1. Light is the most significant sensory medium because it comprises an estimated 85% of sensory input and acts upon the sympathetic and parasympathetic nervous system(s).
2. The EEG frequencies have somatic and psychosomatic significance. The delta and theta frequencies function throughout the 24 hour cycle and must therefore be associated with the body´s continuous 24 hour function (somatic) whereas the gamma, beta and alpha frequencies function mainly during periods of wakenedness (psychosomatic).
Preliminary research has illustrated that, of the psychosomatic frequencies
- The gamma frequency is associated with predictive function and/or subliminal imaging;
- The beta frequency is associated with physical function and sense perception; and
- The alpha frequency is associated with coherent patterns of behaviour i.e. thought and learning. Each functions independently of the other yet influences and is influenced by the other frequency ranges.
- The theta frequencies are associated with pain, photosensitivity, and fixation of memories [7,8]; and
- The delta frequency is associated with sleep (the majority of sleep is in the delta frequency state) and in periods of physiological damage e.g. in the comatose state when the brain shuts down all peripheral activity and focuses upon the delta frequency/state [8,9].
Sleep is a Physiological System
The author has previously presented papers which illustrate that blood pressure, blood glucose and pH exhibit the hallmarks of neurally regulated physiological systems. Sleep also exhibits the hallmarks of a neurally regulated physiological system i.e. it involves the coherent function of a network of organs; however, as outlined above, more than 50% of the deepest stage 4 sleep takes place in the delta state of a healthy patient. This illustrates the immense physiological significance and importance of the delta frequency e.g.
- During sleep, in a healthy patient, the theta and delta frequencies function in a coherent and apparently coordinated manner however, when under stress, the coherent function of theta and delta frequencies can be significantly destabilised [7-9].
- When awake, the beta and alpha frequencies generally function in a coherent manner. Logical behaviour is dependent upon the coordinated function of the different frequency bands however, when under stress, the coherent function of the beta and alpha frequency bands may become stabilised and the patient´s actions less logical. If the person undertakes less physically active tasks e.g. playing computer games, the beta frequency band becomes less significant and the alpha band becomes more significant.
- Memories which are experienced in beta and alpha frequencies are fixed in the theta, and perhaps also the delta, band by the process of LTP. The greater the severity of stress - whether it is experienced as psychological stress, pain, or as damage or degeneration - illustrates the existence of a structured relationship between the psychosomatic and somatic states and between the different EEG frequencies i.e. that each EEG frequency band complements adjacent frequency bands and hence has differing levels of physiological significance [8]. Stress influences the quality and quantity of sleep and the fixation and recall of memories.
In cases of severe or extreme neural trauma e.g. in the comatose state, there is significantly greater periods spent in delta frequency which indicates that the sleep state acts to protect the brain and stimulate or elevate immune function and normal patterns and/or processes of repair, recovery and regeneration [15]. Moreover in such cases the vast majority of sleep can be in delta sleep which indicates that it is a significantly more important state than that of the other frequency bands. Finally, applied frequency/delta sleep (as SLT) has been illustrated to have a significant therapeutic effect [16].
Grakov´s description of the physiological systems considers skin as an organ, which participates in the physiological system ‘optimisation of body temperature’ [Note 5 ]. It does not consider skin to be a system. It does not make allowance for an immune ‘system’ but instead considers that immune ‘function’ is provided by the coherent inter-relationship between different the different physiological systems and organs (spleen, thymus, musculoskeletal, thyroid gland, pituitary gland) which act in a concerted manner to optimise normal function and produce immunoglobulins, cytokines, neutrophils, etc.
It appears reasonable to conclude therefore that changes of EEG frequency appear to be associated with different levels of cell function:
- The delta frequency in particular being associated with the coherent function of the physiological systems and organs and, in particular with damage or degeneration.
- The theta frequencies with cellular damage.
- The alpha frequencies with cellular dysfunction arisingfrom significant levels (frequency or magnitude) of multi-sensory input (psychological stress).
- The beta frequencies are associated with basic sensory input,data collection and/or perception, and
- The gamma frequencies, often associated with subliminal imaging, with predictive significance.
It is reasonable to consider therefore that sleep is a physiological system which comprises a network of organs which has the purposeof ‘assimilating into the neural program information which has been absorbed during the day; preparing the controlling programme for the next day of activity; checking the condition of organs and tissues; and correcting the controlling signals which stimulate the production of hormones’.
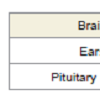
Grakov has identified the nature and significance of the autonomic nervous system and physiological systems, in particular the organs which are part of each physiological system. As an example, the sleep system comprises the following organs (Table 2), and that emergent pathologies (which may be genetic or phenotypic or a combination of both) in any of these organs e.g. nasal problems affecting breathing, hearing problems, spinal cord damage, pituitary problems, and the peripheral nervous system, can be expected to directly influence the quality and quantity of sleep [17]. This is immensely significant in cases where impaired sleep is a common symptom e.g. of stress, depression, Alzheimer´s disease, etc [18-24]. A lack of adequate quality or quantity of sleep is associated with a plethora of medical conditions e.g. diabetes, cardiovascular disease, cancer(s), etc [25-27].
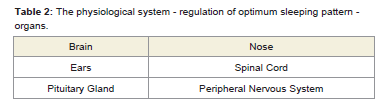
Table 2: The physiological system - regulation of optimum sleeping pattern - organs.
It supports the contention that sleep has biochemical/pathological significance and that it plays a fundamental role eliminating the body of toxins or pathological metabolites which accumulate during eriods of physical activity or inactivity, consolidating memories, elevating the production of immunochemicals, and perhaps also changing the way in which memories of different levels of significance are stored [29].
Sleep has an anti-inflammatory role upon cell function which assists the body´s natural eliminatory process(es), mainly via the urinary tract and lymphatic ducts, to eliminate toxins and thereby optimise normal cell function [11,12]. This is supported by noting that the brain shrinks in size during periods of sleep [30].
It offers a viable explanation for the many and various drug side-effects arising from use of benzodiazepines, zopiclone, and other drugs which are often used to treat hypersomnia (apnoea) or hyposomnia (insomnia) e.g. blurred vision, incontinence, dry mouth, constipation, drowsiness, instability, osteoporosis, heartburn, etc.
It explains why common approaches adopted by the medical profession included stressing/teach relaxation/yoga/meditation, and ‘retraining the brain’ into more acceptable or typical sleep patterns.
The recognition that immune ‘function’ is provided by the coherent inter-relationship between different the different physiological systems and organs; which act in a concerted manner to optimise normal function and produce immunoglobulins, cytokines, neutrophils; is intriguing because an investigational study compiled by Zhuravleva TN and Komarova IA of the Laboratory of Molecular Cosmetology (Mirra-Lux-Ltd, Moscow) illustrated that SLT (see section 4) was able to stimulate the immune response in 34 patientsas follows:
Intention of the study: Number of patients: 34 (17 male and 17 female within 17-60 yrs)
1. To investigate blood content and immune status using contemporary diagnostic tests.
2. To carry our correctional therapy using Strannik Light Therapy (SLT).
3. To check immune status using contemporary diagnostic tests.
4. To check/compare initial SVS results before and after correctional therapy
Results
1. The level of immunoglobulins IgG, IgA, IgM determined using the Mancini technique was within the normal reference range for all patients.2. The total lymphocytes was within the normal reference range at the first investigation but increased by circa 50% after correctional therapy (SLT).
3. Phagocytosis activity of neutrophils was within normal limits at the first investigation (1.42) and increased by 10% (1.53) after correctional therapy (SLT).
4. The level of neutrophil lysosomal-cationic proteins identifying non-enzymatic bactericidal activity ofgranulocytes, determined using Shubitch MG method: at the first investigation average cytochemical coefficient (ACC) was at a low level of 1.35. After correctional therapy (SLT) this increased to a level of 1.61 which was within the normal reference range 1.50-1.70.
5. The level of lymphocytes was measured by an indirect fluorescence staining immunoassay method using monoclonal antibodies. Each patient had CD3, CD4 and CD16 levels within the normal reference range before and after correctional therapy (SLT) although slightly elevated after correctional therapy.
6. Patients reported, following correctional therapy (SLT), lower levels of tiredness, improved health andresistance to viral infection. Patients with high blood pressure (4) stabilised their blood pressure at normal age-related levels and reported improved sleeping patterns.
In addition the author reports two case studies which illustrate how Strannik Virtual Scanning (SVS) technology has been able to determine the onset and progression of immune-related pathologies and how such conditions have responded to correctional therapy (SLT):
Case study 1
In a patient who had required a bone marrow transplant as a result of chemotherapy treatment for her acute myeloblastic anaemia, the patient was tested by contemporary diagnostic tests which concluded that the patient´s condition was normal however SVS identified the likely reoccurrence of such a condition which was reconfirmed at the patient´s following medical condition. SVS was able to determine the condition earlier than contemporary diagnostic tests.
Case study 2
In an elderly patient with thrombocytopenia/atypical leucaemia, his thrombocyte count rose during a course of correctional therapy (SLT) from circa 60,000 to circa 125,000 platelets per micro liter of blood over a period of circa 2 months. The normal reference range is 150,000 to 450,000 platelets per micro liter of circulating blood.
Strannik Software
Strannik software is the first of a new generation of medical technology to meet the key aims and objectives of the Human Brain Project. It arose out of fundamental research into the medical application of industrial lasers by the brilliant researcher Dr. Igor Gennadyevich Grakov and culminated in an understanding of the fundamental mechanism which has been adopted by the brain to regulate the body´s function. It comprises Strannik Virtual Scanning (SVS) and Strannik Light Therapy (SLT).
Strannik virtual scanning
SVS is able to screen the health of the patient in an apparently extraordinary level of detail i.e. at the level of the physiological systems determining the most destabilised physiological systems, at the organ level determining the most destabilised organs, at the cellular level determine the extent of cellular change which is significant in cancer screening, and at the molecular or pathological level where the technique can determine the extent of the genetic and phenotypic processes in each emergent pathological process (typically 15 pathologies per organ in circa 30 organs) (see Figures 1-3).
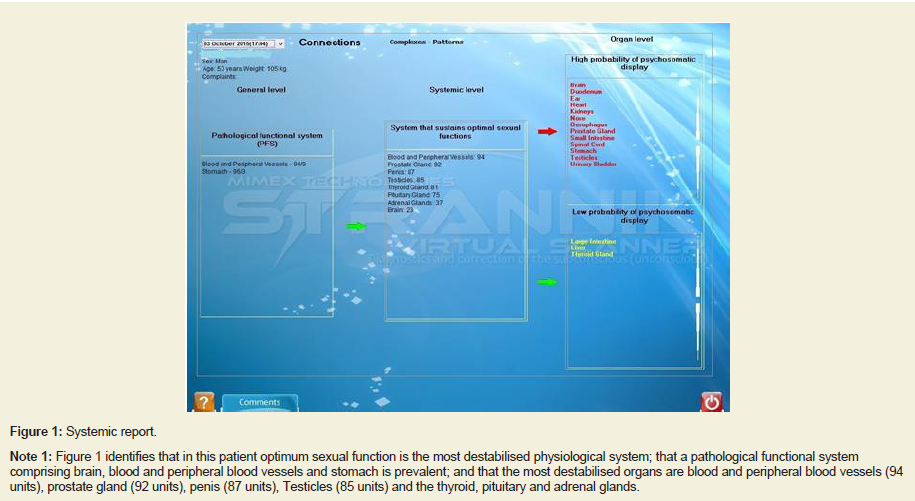
Figure 1: Systemic report.
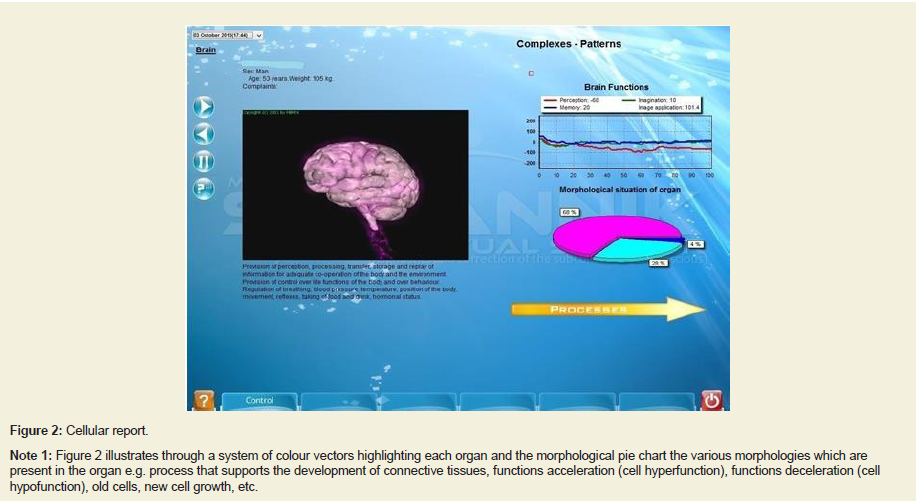
Figure 2: Cellular report.
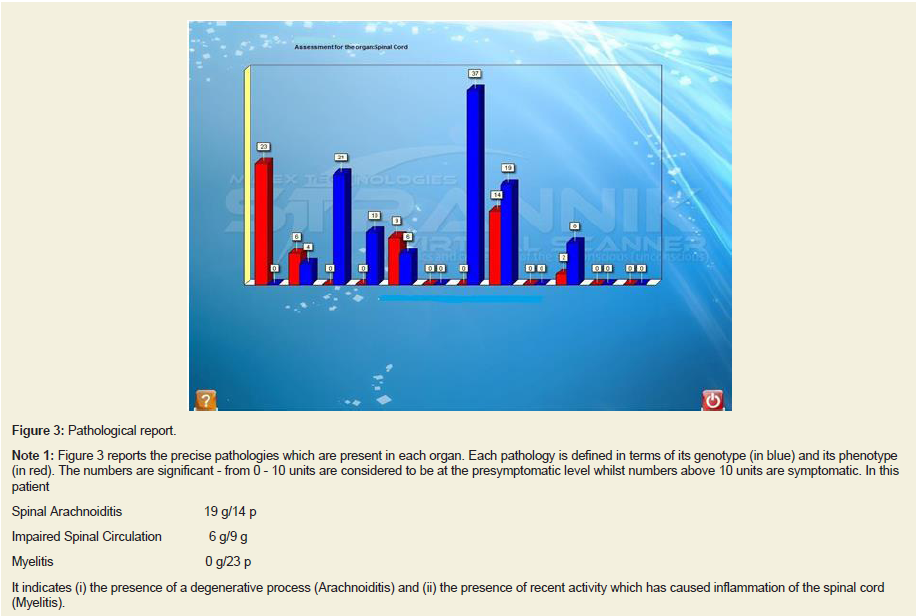
Figure 3: Pathological report.
Strannik light therapy
The knowledge, embodied in SLT, of how the brain deploys light and frequency in order to regulate the body´s function has largely baffled and defeated researchers. There is some degree of understanding of the phenomena but not an in - depth level of knowledge. Accordingly the results obtained by the many and various techniques, which are based on limited levels of understanding, are often less than claimed or expected thereby leading to doubts over the significance of the phenomena and occasionally allegations of impropriety. By comparison, SLT is the first technology to be based upon a precise understanding, embodied in a mathematical model, enabling accurate selection of the therapeutic parameters.
Initial research suggests that SLT performs at circa 83-96% effectiveness depending upon the nature and extent of the morbidities to be treated [16]. Such levels of reported effectiveness appear consistent with an estimated 4-17% of patients with genetic conditions, or physical damage or degeneration, which would not be expected to respond to a therapy which is based upon correcting autonomic dysfunction.
Case Studies
SVS has proven to be an extremely effective way of determining the physiological systems which are most dysfunctional in patients e.g. it routinely identifies when patients have poor levels of sleep, have problems with blood pressure or blood glucose, etc.
- Initial research has indicated that SVS appears to function at a level which is typically 2-23% more accurate than the entire range of contemporary diagnostic tests in use at the various hospitals which have evaluated the technology and against which it was compared e.g. a demonstration to the Medical Director of Nottingham´s Queens Medical Center in 2003 illustrated how the technology was able to determine, precisely, the range of 5-6 ailments of concern to the selected test patient. The MD commented that the entire QMC did not have the capability to perform at this level.
- As outlined earlier, initial research has indicated that SLT appears to function at a level which is typically 83-96% effective treating 30 different categories of common ailments. Case Studies recorded by Mimex Montague Healthcare support such claims that the technology works at this general level of effectiveness - it treats or corrects autonomic dysfunction - but that the calculation of outcome of effectiveness following treatment will ultimately depend upon the precise nature of the conditions to be treated. SLT has not proven to be effective when used to treat Chronic Fatigue Syndrome which suggests that this medical condition has genetic origins, perhaps resulting from a viral infection.
Case study 3: Female, circa 60 years, retired senior nursing officer/matron; insomniac, completely unable to sleep following an operation to remove a brain tumour several years previously. After 1 - 2 weeks of SLT she phoned to enquire whether sleeping 12-14 hoursper day was normal.
Case study 4: Male, circa 60 years; with sleep apnoea, being treated with oxygen, falling asleep throughout the day; was successfully treated with SLT over several months to the extent that his specialist advised during a routine follow-up consultation that the patient no longer suffered from sleep apnoea.
Case study 5: Male, circa 60 years; periodically experiences lack of sleep and/or disruption to sleeping patterns, in particular the ability to fall asleep, to remain asleep throughout the night, and/or sleep for 8 hours. Problem associated with stress which was linked to business issues. Routinely uses SLT to deal with the problem.
Further case studies outlining the effectiveness of SLT are listed on the company´s web site "www.montaguehealthcare.co.uk"
Discussion
The author reports that disorders of the physiological system ‘optimum sleeping pattern´ responds exceptionally well to SLT with circa 100% outcomes in patients treated since 2003. Sleep dysfunction is a commonly observed phenomena in patients with stress; and/or abnormalities of, or damage to, or degeneration of the brain, spinal cord, and adrenal gland. Sleep dysfunction due to damage or degeneration may respond favourably to a course of SLT but eradication of the symptom, and complete recovery of normal sleeping patterns, depends upon the physiological origins of the condition.It highlights the dynamic relationship between the function of the brain to regulate the autonomic nervous system and stable and coherent function of the organ networks; and the various factors, such as stress or pathological onset, which influence this dynamic relationship.
The hypothesis outlined in this paper - that the brain regulates the body´s function - is supported by issues/observations identified by many eminent and immensely respected researchers e.g. Lander [Note 6 ], Brenner, Kandel, Noble, etc [37-39]; for a comprehensiveunderstanding of how the body functions………
- ‘We have the parts list but need the operating manual’ (Lander [Note 6 ]).
- Top-down, bottom-up, middle-out´ (Brenner [37]).
- The need to consider and/or incorporate sensory input in research studies alongside biomedical research (Kandel [38]).
- ‘Linking molecular biology, cellular biology, organ function and system function’ (Noble [37,39]).
The authors, in this and other published papers, point out the limitations of the prevailing medical paradigm which (i) seeks to identify a single pathological process as the fundamental cause of a medical condition and then to treat this single pathological process with a drug which blocks or otherwise acts to modulate the effect of the emergent pathological process i.e. by effectively acting against the neural regulation of system function; (ii) to ignore that stress is primarily experienced through multi-sensory input, at different levels of physiological significance, and is ultimately manifest as a complex spectrum of pathological correlates; and (iii) that the body´s function is neurally regulated and acts to compensate for sensory and biological input.
This illustrates that pathological onset is the consequence of neural dysfunction which influences the stable and coherent function of the organ networks; that stress in its many and various guises is often (estimated 80-90%)the fundamental cause of the problem; and finally that the brain uses applied frequencies to re-establish normal levels of brain function, including the learning process.
Such a hypothesis meets the primary aims and objectives of the Human Brain Project i.e. (i) to identify what the brain does and how it does it, (ii) to adapt this knowledge to develop a new generation of cognitively-based diagnostic techniques which are able to determine the pathological correlates of complex conditions such as Alzheimer´s disease, and (iii) to understand and adapt with therapeutic effect a multi-level understanding of how the brain functions.
Conflict of Interest
Graham Ewing is Chief Executive Officer, Mimex Montague Healthcare which has the sole purpose of commercialising Stranniktechnology.Notes
- https://www.humanbrainproject.eu
- http://www.scientificamerican.com/article/what-is-thefunction-of-t-1997-12-22/
- http://merckbooks.com/mmanual/index.html
- http://www.pbs.org/wgbh/nova/genome/deco_lander.html
- www.montaguehealthcare.co.uk/OperatingManual.pdf
- http://www.pbs.org/wgbh/nova/genome/deco_lander.html
Acknowledgements
The author wishes to thank the many researchers who through their research have indirectly contributed to this paper.References
- Billiau AD, Witters P, Ceulemans B, Kasran A, Wouters C et al. (2007) Intravenous immunoglobulins in refractory childhood-onset epilepsy: effects on seizure frequency, EEG activity, and cerebrospinal fluid cytokine profile. Epilepsia 48: 1739-1749.
- Castellani G, Intrator N, Remondini D (2014) Systems biology and brain activity in neuronal pathways by smart device and advanced signal processing. Front Genet 5:253.
- Ewing GW (2012) pH is a physiological system. Increased acidity alters protein conformation and cell morphology and is a significant factor in the onset of diabetes and other common pathologies. Open Syst Biol J 5: 1-12.
- Noakes TD, St Clair GA, Lambert EV (2004) From catastrophe to complexity: a novel model of integrative central neural regulation of effort and fatigue during exercise in humans. Br J Sports Med 38: 511-514.
- St Clair GA, Noakes TD (2004) Evidence for complex system integration and dynamic neural regulation of skeletal muscle recruitment during exercise in humans. Br J Sports Med 38: 797-806.
- Ewing GW, Parvez SH (2010) The dynamic relationship between cognition, the physiological systems, and cellular and molecular biochemistry: a systems-based perspective on the processes of pathology. Act Nerv Super Rediviva 52: 29-36.
- Doose H, Baier WK (1988) Theta rhythms in the EEG: a genetic trait in childhood epilepsy. Brain Dev 10: 347-354.
- Lømo T (2003) The Discovery of Long-term Potentiation. Philos Trans R Soc Lond B Biol Sci 358:617-620.
- van Dongen EV, Takashima A, Barth M, Zapp J, Schad LR, et al. (2012) Memory stabilization with targeted reactivation during human slow-wave sleep. Proc Natl Acad Sci 109: 10575-10580.
- Belenky G, Wesensten NJ, Thorne DR, Thomas ML, Sing HC, et al. (2003) Patterns of performance degradation and restoration during sleep restriction and subsequent recovery: a sleep dose-response study. J Sleep Res 12: 1-12.
- Meinhardt U, Nelson AE, Hansen JL, Birzniece V, Clifford D, et al. (2010) The effects of growth hormone on body composition and physical performance in recreational athletes: a randomized trial. Ann Intern Med 152: 568-577.
- Tan DX, Manchester LC, Reiter RJ, Qi WB, Karbownik M, et al. (2000) Significance of melatonin in antioxidative defense system: reactions and products. Biol Signals Recept 9: 137-159.
- Brabant G, Prank K, Ranft U, Schuermeyer T, Wagner TO, et al. (1990) Physiological regulation of circadian and pulsatile thyrotropin secretion in normal man and woman. J Clin Endocrinol Metab 70: 403-439.
- Bellastella A, De Bellis A, Bellastella G, Esposito K (2013) Opposite influence of light and blindness on pituitary-gonadal function. Front Endocrinol (Lausanne) 4: 205.
- Beridze M, Khaburzania M, Shakarishvili R, Kazaishvili D (2010) Dominated EEG patterns and their prognostic value in coma caused by traumatic brain injury. Georgian Med News 186: 28-33.
- Vysochin YV, Lukoyanov VV, Yaichnikov IK, Tkachuk MI, Chyev VA, et al. (2000) Methodology and technology of invigoration of different population orders. In: consolidated 5 year research plan of physical training, sports and tourism state committee of the Russian Federation.
- Romijn JA (2016) Pituitary diseases and sleep disorders. Curr Opin Endocrinol Diabetes Obes 23: 345-351.
- Cevizci R, Kemaloglu YK, Yilmaz M, Duzlu M, Karamert R (2016) Role of nasal problems on positional and nonpositional obstructive sleep apnea. Kulak Burun Bogaz Ihtis Derg 26: 219-224.
- Test T, Canfi A, Eyal A, Shoam-Vardi I, Sheiner EK (2011) The influence of hearing impairment on sleep quality among workers exposed to harmful noise. Sleep 34: 25-30.
- Jensen MP, Hirsch AT, Molton IR, Bamer AM (2009) Sleep problems in individuals with spinal cord injury: frequency and age effects. Rehabil Psychol 54: 323-331.
- Schmidt S, Rodrigues A, Lupi ME, Wong F (2013) Peripheral neuropathy linked to obstructive sleep apnea? J Fam Pract 62: 577-578.
- Kuem SH, Lin K, Insop S (2012) Stress and Sleep Disorder. Exp Neurobiol 21: 141-150.
- Hasler BP, Buysse DJ, Kupfer DJ, Germain A (2010) Phase relationships between core body temperature, melatonin, and sleep are associated with depression severity: further evidence for circadian misalignment in non-seasonal depression. Psychiatry Res 178: 205-207.
- Mander BA, Marks SM, Vogel JW, Rao V, Lu B, et al. (2015) β-amyloid disrupts human NREM slow waves and related hippocampus-dependent memory consolidation. Nat Neurosci 18: 1051-1057.
- Kawakami N, Takatsuka N, Shimizu H (2004) Sleep disturbance and onset of type 2 diabetes. Diabetes Care 27: 282-283.
- Wolk R, Gami AS, Garcia-Touchard A, Somers VK (2005) Sleep and cardiovascular disease. Curr Probl Cardiol 30: 625-662.
- Roscoe JA, Kaufman ME, Matteson-Rusby SE, Palesh OG, Ryan JL, et al. (2007) Cancer-related fatigue and sleep disorders. Oncologist 12: 35-42.
- Zhang J, Zhu Y, Zhan G, Fenik P, Panossian L, et al. (2014) Extended wakefulness: compromised metabolics in and degeneration of locus ceruleus neurons. J Neurosci 34: 4418-4431.
- Ackermann K, Revell VL, Lao O, Rombouts EJ, Skene DJ, et al (2012) Diurnal rhythms in blood cell populations and the effect of acute sleep deprivation in healthy young men. Sleep 35: 933-940.
- Sexton CE, Storsve AB, Walhovd KB, Johansen-Berg H, Fjell AM. Poor sleep quality is associated with increased cortical atrophy in community-dwelling adults. Neurology 83: 967-973.
- Ewing GW (2016) Further perspectives on diabetes: neuroregulation of blood glucose. Neurosci Bio-med Eng 4: 1-9.
- Ewing GW, Ewing EN (2009) Computer diagnosis in cardiology. N Am J Med Sci 1: 152-159.
- Ewing GW, Ewing EN. Virtual Scanning - a new generation of medical technology - beyond biomedicine? pub Montague Healthcare books, pp. 246.
- Ewing GW (2016) The use of strannik virtual scanning as a modality for the earliest screening of the pathological correlates of alzheimer´s disease. Human Frontier Science Program (HFSP) Journal 10: 2-20.
- Ewing GW (2015) Case study: the determination a complex multi-systemic medical condition by a cognitive, virtual scanning technique. Case Rep Clin Med 4: 209-221.
- Ewing GW, Duran JC (2016) A report of the ability of strannik virtual scanning to screen the health of a randomly selected cohort of patients. Enliven: Neurol Neurotech 2: 01.
- Complexity in biological information processing. Bock G, Goode J (Eds), John Wiley & Sons, Ltd.
- Kandel ER (2006) Essay: The new science of mind. Sci Am Mind 17: 62-69.
- Noble D (2008) Claude Bernard, the first system biologist, and the future of physiology. Exp Physiol 93: 16-26.