
International Journal of Otorhinolaryngology
Download PDF
Case Report
*Address for Correspondence: Abbas Younes, MD FACS, Assistant Professor of Surgery & Pediatrics, Department of Otolaryngology-Head & Neck Surgery, University of Kentucky Chandler Medical Center, University of Kentucky, 800 Rose Street, C236, 800 Rose Street, C236, USA, Tel: 859-218-2143; E-mail: abbasyounes@hotmail.com
Citation: Alfonso K, Younes A. The Eight Year Nasal Foreign Body: A Case Report. Inter J Otorhinolaryngology. 2015;2(1): 2.
Copyright © 2015 Younes et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolarygology | ISSN: 2380-0569 | Volume: 2, Issue: 1
Submission: 01 July 2015 | Accepted: 21 July 2015 | Published: 24 July 2015
 He was taken to the operating room. The granulation tissue was involving the anterior aspect of the middle turbinate. Excision of granulation tissue was completed and a foreign body was encountered ( Figure 2). The caudal middle turbinate was resected secondary to adherence of the foreign body and granulation tissue. Maxillary antrostomy was performed.
He was taken to the operating room. The granulation tissue was involving the anterior aspect of the middle turbinate. Excision of granulation tissue was completed and a foreign body was encountered ( Figure 2). The caudal middle turbinate was resected secondary to adherence of the foreign body and granulation tissue. Maxillary antrostomy was performed.
 On his two-week postoperative appointment, he noted improvement of breathing and epistaxis. Rigid nasal endoscopy revealed well healed mucosa with patent middle meatus. No further evidence of granulation tissue or mucopurulence remained.
On his two-week postoperative appointment, he noted improvement of breathing and epistaxis. Rigid nasal endoscopy revealed well healed mucosa with patent middle meatus. No further evidence of granulation tissue or mucopurulence remained.
The Eight Year Nasal Foreign Body: A Case Report
Kristan Alfonso and Abbas Younes*
- Department of Otolaryngology-Head & Neck Surgery, University of Kentucky Chandler Medical Center, University of Kentucky, USA
*Address for Correspondence: Abbas Younes, MD FACS, Assistant Professor of Surgery & Pediatrics, Department of Otolaryngology-Head & Neck Surgery, University of Kentucky Chandler Medical Center, University of Kentucky, 800 Rose Street, C236, 800 Rose Street, C236, USA, Tel: 859-218-2143; E-mail: abbasyounes@hotmail.com
Citation: Alfonso K, Younes A. The Eight Year Nasal Foreign Body: A Case Report. Inter J Otorhinolaryngology. 2015;2(1): 2.
Copyright © 2015 Younes et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolarygology | ISSN: 2380-0569 | Volume: 2, Issue: 1
Submission: 01 July 2015 | Accepted: 21 July 2015 | Published: 24 July 2015
Introduction
Nasal foreign bodies are common place in pediatric otolaryngology. They occur most commonly in the age group ranging from 2 to 5 years of age with an equal sex predilection. Infants develop pincer grasp around the age of 9 months, and this is typically the youngest patient a nasal foreign body will present in. Typical presentation includes unilateral nasal obstruction with foulsmelling, chronic unilateral nasal drainage [1]. The object itself causes little to no pain. It is most frequently lodged just caudal to the middle turbinate or along the floor of the nose, under the inferior turbinate. Length of time to diagnosis is typically short, with one study showing that nearly 75% of cases present within 24 hours [2]. Another showed similar results with 80% presenting within 24 hours and only 10% with delayed presentation [3]. However, reports have shown it may even take years in asymptomatic individuals [4]. A variety of objects are found, most commonly easily-acquired household entities. These can cause dangerous sequelae, like orbital infections, meningitis or tetanus. Batteries can cause severe mucosal injury and are considered emergencies. Case reports also describe iatrogenic materials, like packing, being found many years later [5]. In this case report, we present an 11-year-old male with an 8-year symptomatic history of nasal foreign body.Keywords
Nasal foreign body; Chronic rhinosinusitisCase Report
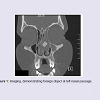
IRB exception was granted by the University of Kentucky office of Research Integrity. An 11-year-old male presented in the ambulatory setting with a history of chronic purulent nasal drainage. His mother explained that his symptoms started at age 3. They included chronic, foul-smelling nasal drainage only from the left nasal passage. He had difficulty breathing through his nose and was constantly mouth breathing. His smell and taste were diminished. He also had epistaxis nearly daily from the left nasal passage. He had been treated for years with courses of antibiotics. He did not have any significant past medical history, including no history of pneumonia, aspirin sensitivity or asthma. He had never been tested for cystic fibrosis. He took no medications on a regular basis and did not have allergies. After the failure of medical treatment, the primary care physician ordered a CT scan of sinuses, and referred the patient to our clinic.On physical exam, the patient demonstrated mouth-breathing. He had no evidence of external nasal deformity. He had right septal deviation with thick, left-sided mucopurulence. On endoscopy, the left nasal passage had evidence of obstructive granulation tissue. His exam was otherwise benign. The recently performed CT scan was reviewed with an estimated a 1 cm foreign body within the left nasal canal that was causing occlusion of the OMC. He had opacification of the left ethmoid frontal and maxillary sinuses ( Figure 1).
Figure 1: Imaging, demonstrating foreign object at left nasal passage.

Figure 2: Specimen.
Discussion
This case reports demonstrates the classic presentation of nasal foreign body. Interestingly, this patient had been undiagnosed for 8 years in which he was treated with chronic antibiotics by primary care. His nasal anatomy had developed around the foreign body, leading to significant septal deviation and nasal obstruction. This case demonstrates the importance of early diagnosis and management of nasal foreign bodies to prevent chronic morbidity and late sequelae. It stresses the fact that we need to educate our pediatricians to suspect and investigate the possibility of nasal foreign body when a child presents with history of unilateral obstruction and chronic foul smelling drainage. This should prompt early referral to us for nasal endoscopy in the clinic.References
- Kalan A, Tariq M (2000) Foreign bodies in the nasal cavities: a comprehensive review of the aetiology, diagnostic pointers, and therapeutic measures. Postgrad Med J 76: 484-487.
- Tong MCF, Ying SY, Van Hasselt CA (1996) Nasal foreign bodies in children. Int J Pediatr Otorhinolaryngol 35: 207-211.
- Mackle T, Conlon B (2006) Foreign bodies of the nose and ears in children. Should these be managed in the accident and emergency setting? Int J Pediatr Otorhinolaryngol 70: 425-428.
- Tay AB (2000) Long-standing intranasal foreign body: an incidental finding on dental radiograph. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 90: 546-549.
- Kelesidis T, Osman S, Dinerman H (2010) An unusual foreign body as cause of chronic sinusitis: a case report. J Med Case Rep 4: 157.